ADDRI is an independent, not-for-profit research institute committed to reducing and ultimately eliminating the impact of asbestos and dust-related diseases worldwide.
Our team of doctors, researchers, scientists, nurses and industry leaders excel in innovative thinking and strive for excellence every day.
The importance of collaboration
We are on a mission to collaborate with those working toward the elimination of asbestos and dust-related diseases.
About the Diseases
Asbestos and dust diseases remain a clear and present danger. 4,000 Australians die each year from asbestos-related diseases. It is estimated that one in four workers are at risk of silica-related disease.
Asbestos is a type of mineral made up of tiny, needle-like fibers. Known for its ability to resist heat, electricity, and corrosion, it was widely used in many construction materials. Inhalation of asbestos fibres can directly lead to disease and a form of cancer called mesothelioma.
What is Silica?
Crystalline silica is a natural mineral found in sand, stone, concrete and mortar. Found in high quantities in materials commonly used for tunnel construction and engineered stone, inhalation of silica dust particles can cause serious disease.
Research
We are on a mission to understand asbestos and dust-related disease development and diagnosis through dedicated research. Our evidence-led research drives advancements in medical and scientific understanding and guides our global education and training initiatives.
We are unrelenting in exploring every avenue that will achieve our mission of improving patient outcomes, uncovering new treatments and ultimately ending all asbestos and dust-related diseases.
Working globally
Our status as the WHO Collaborating Centre for Elimination of Asbestos-Related Diseases ensures that our dedication, research and collaboration will have significant impact around the world.
Support
We are on a mission to support people impacted by dust-related diseases. Our Mesothelioma and Silicosis Support Service addresses the needs of patients suffering dust-related diseases and supports their families.
Our specialist nurses are here to address the needs of our patients with mesothelioma and to support carers and families. We can answer any questions you may have and help you navigate the health system
Silicosis support
Emotional and practical support for individuals diagnosed with silicosis and their caregivers.
Education
We are on a mission to educate that asbestos is a very real threat to people all over the world and provide the knowledge and tools to care for those impacted.
An internationally recognised eToolkit on asbestos-related diseases (ARDs), important research to fill knowledge gaps on the elimination of asbestos and much needed training on ARDs in developing countries.
Mesothelioma learning module
Access online training for nurses/health care professionals to assist with diagnosing and caring for patients with mesothelioma.
Malignant Pleural Mesothelioma (MPM) is an aggressive malignancy that arises from the mesothelioma surfaces of the pleural cavity. Predominately associated with asbestos, this illness is diagnosed often many decades after initial exposure. Despite legislation against the use of blue asbestos in 1978, and an Australia wide ban on chrysotile asbestos in 2003, Australia is only now seeing evidence of an incidence peak. Furthermore, ongoing exposure to asbestos in the domestic setting, particularly amongst tradesmen and home renovators, will see ongoing diagnoses of this malignancy for decades to come. In the developing world, where significant ongoing industrial and household use of asbestos remain MPM, amongst other asbestos related diseases (ARDs) will continue to surge.
A practical approach to the management of MPM is required encompassing systemic therapy, radiation therapy, surgical intervention and palliative care.is essential. We highlight current best practice and the evidence supporting the use of anti-cancer and supportive therapies, acknowledging the ‘gold standard’ for optimal care in addition to realistic and feasible interventions that are recommended in resource-poor regions.
Systemic Therapies
Systemic therapies have an important role in the management of unresectable malignant mesothelioma. Since 2003, several large randomised trials have reported survival benefit and improved quality of life (QoL) with the use of cisplatin and pemetrexed in MPM, which is now considered the standard of care in those with good performance status and adequate organ function (1) Carboplatin in combination with pemetrexed is a reasonable alternative- especially for those who are older or with co-morbidities precluding use of cisplatin. Few alternative systemic treatment options yield response rates exceeding 20% in phase II trials (2).
Combination Chemotherapy with Cisplatin (or Carboplatin) and Pemetrexed
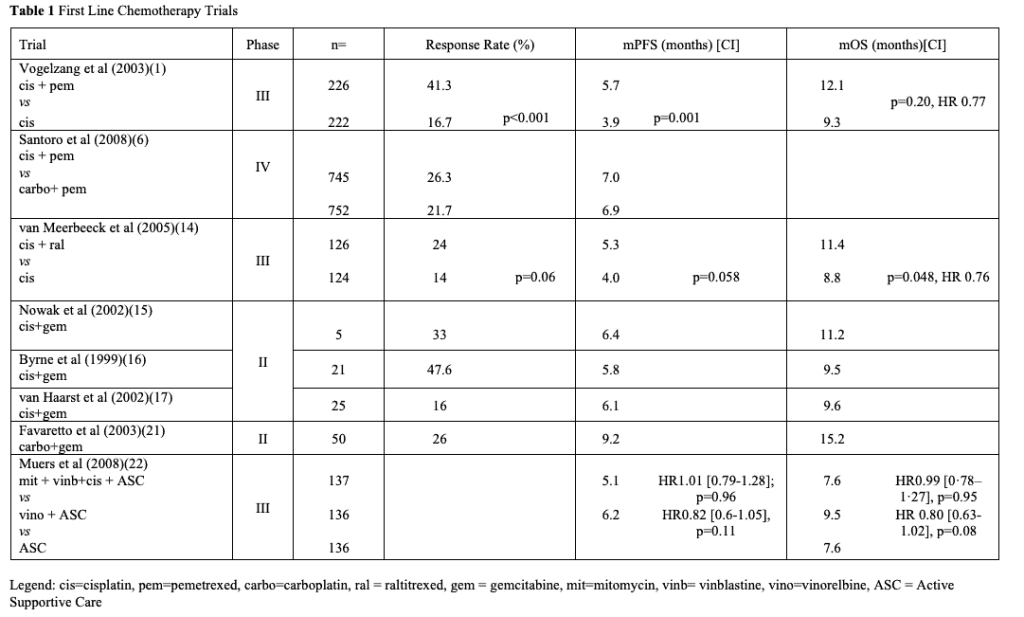
The current standard of care for MPM was established following the results of a large phase III trial by Vogelzang et al. in 2003, which compared combination chemotherapy with cisplatin and pemetrexed, with vitamin B12 and folate supplementation (1). In this trial, 456 chemotherapy-naïve patients with MPM were randomized to cisplatin (75 mg/m2) and pemetrexed (500 mg/m2) given every 3 weeks, or cisplatin alone. Those receiving cisplatin and pemetrexed had a longer median OS (12.1 vs 9.3 months, p=0.02), longer time to progression (5.7 vs 3.9 months p=0.001) and higher objective response rate (41 vs 17%, p<0.0001) compared to cisplatin alone. Those who were also supplemented with oral folic acid and intramuscular vitamin B12 had improved survival, less treatment-related haematological toxicity and received a greater mean number of cycles of treatment.
Quality of life and symptoms were also assessed through the LCSS-Meso questionnaire which had been previously validated MPM (3). Patients who received the combination treatment had statistically significant improvements in symptoms (pain, cough, dyspnoea) by cycle 4, and global QoL and fatigue by cycle 6 (4). Analysis from this trial also identified good performance status, early disease stage, epithelioid histological subtype and non-elevated total white cell count as independent prognostic factors.(5)
Carboplatin is a reasonable alternative for cisplatin in combination with pemetrexed in patients with contraindications to cisplatin. Outcomes for patients who received pemetrexed (500mg/m2) in combination with cisplatin (75mg/m2) or carboplatin (AUC 5) were similar in those enrolled into the International Expanded Access Program(6). Median time to progressive disease was 7 vs. 6.9 months, 1 year survival rates were 63.1% vs 64% and overall response rates 26.3 vs 21.7%.
There have also been three non-randomised Phase II trials evaluating the role of carboplatin and pemetrexed in patients with MPM. Median OS in these three trials range between 12.7 – 14 (7-9). A combined analysis of two of these trials found that the combination of carboplatin and pemetrexed was well tolerated and had similar efficacy in elderly patients (>70 years) compared with younger patients with MPM (10).
Duration and Timing of Chemotherapy
The optimal duration of treatment has not yet been defined, but a commonly used standard for first-line treatment of patients receiving cisplatin (or carboplatin) and pemetrexed is a maximum of six cycles. The median number of cycles of cisplatin and pemetrexed in the seminal Vogelzang et al. 2003 was six, with only 5% of patients tolerating ³ 8 cycles. There is no randomised evidence to show that four cycles of chemotherapy are sufficient.
The feasibility of maintenance pemetrexed after induction chemotherapy was explored in a small non-randomised study in 2006(11). This study found good tolerability of maintenance pemetrexed, with low rate of Grade 3 or 4 toxicities, however was underpowered to investigate treatment response or patient survival.
Following this, a randomised phase II study(12) administered maintenance, single agent pemetrexed vs. observation until disease progression after 4-6 cycles of combination pemetrexed with platinum chemotherapy. Patients in the treatment arm received a median of 4 extra cycles of pemetrexed until disease progression – however, there was no benefit in median progression free survival (median 3.0 vs 3.4 months, HR 0.99, CI 0.51-190, p = 0.9733), nor OS (11.8 vs. 16.3 months, HR 0.86, CI 0.44-1.71, p = 0.6737). Therefore, maintenance pemetrexed is not part of standard clinical practice for MPM.
The timing to start palliative chemotherapy is important as the clinical course of patients with mesothelioma varies widely from indolent to rapidly progressive disease. It is reasonable to consider a period of careful observation with clinical and radiological review before commencing palliative systemic therapy in asymptomatic patients with good prognostic features including epithelioid histology subtype and low tumour volume.
There has been one randomised study of chemotherapy delivered at diagnosis or delayed until symptomatic progression in MPM. This underpowered trial did not show statistically significant difference in OS (14 vs 10 months, p=0.1) nor difference in QoL or symptom outcomes (13). It is important to note that the chemotherapy used in this study (mitomycin, vinblastine and cisplatin) is no longer considered standard of care treatment.
Alternative Cytotoxic Regimens
There are few effective alternative options to first line combination cisplatin (or carboplatin) and pemetrexed chemotherapy. The combination of cisplatin with raltitrexed or gemcitabine could be considered only if pemetrexed was contraindicated or unavailable.
A randomised phase III trial by van Meerbeeck et al. in 2005 compared cisplatin (80mg/m2) alone, or in combination with raltitrexed (3mg/m2) in 250 chemotherapy-naïve patients with MPM. In this trial, median OS was reported to be improved significantly (11.4 vs 8.8 months p=0.048), and higher response rates (24 vs. 14%, p=0.06). The difference in progression free survival was not statistically significant (5.3 vs 4 months(14).
The combination of cisplatin and gemcitabine has been evaluated in several small phase II trials as first-line combination chemotherapy for MPM. Reported response rates ranged from 12-48% and median OS 9.5-12 months (15-19). The combination of carboplatin and gemcitabine has also been evaluated in a multi-centric Phase II study (20) with comparable response rate (26%) and median survival (66 weeks) to combination with cisplatin.
Table 1. First Line Chemotherapy Trials
Treatment of Relapsed Mesothelioma (2nd line treatment and beyond)
Many patients with MPM who benefit from first line treatment are still relatively fit at time of radiological disease progression and potentially could receive further treatment. Chemotherapy beyond first line treatment is less well-studied and the optimal regimen is unknown. In developing nations where availability of first line agents is limited, suitable second line options remain minimal.
Pemetrexed Naive, but Previously Treated Patients
In previously treated, but pemetrexed-naïve patients with relapsed MPM, a pemetrexed containing regimen should be considered in the second-line.
An observational study by Janne et al. (2006) reported outcomes of 153 pemetrexed naïve patients with MPM who received pemetrexed based chemotherapy via an access program in the second line setting(23). Patients receiving combination pemetrexed plus cisplatin or pemetrexed alone had similar rates of stable disease (36.3% and 41.1%, respectively), however higher rates of treatment response occurred in those receiving combination therapy (32.5%, compared with 5.5% for single-agent pemetrexed).
These findings were confirmed in a phase III trial by Jassem et al. (2008) (24) comparing pemetrexed 500mg/m2 and best supportive care (BSC) with BSC alone in 243 patients with previously treated but pemetrexed-naïve patients with relapsed MPM. Response rate significantly favoured the pemetrexed arm (18.7 vs 1.7%, p<0.001) and median PFS was also longer in the pemetrexed arm (3.7 vs 1.5 months, p=0.0148). There was no statistically significant difference in QoL assessments nor in OS (8.4 vs 9.7 months, p=0.0148) – although these may have been confounded by the significant proportion of patients receiving chemotherapy after trial discontinuation (35% in pemetrexed arm vs. 51.7% in BSC arm).
Zucali et al. 2011(25) published a retrospective of 423 patients who received second line treatment for MPM between 1996-2008. With second line treatment, 52.6% achieved disease control, median PFS 4.3mo, OS 8.7 months. According to multivariate analysis, disease control after second line therapy was related significantly to pemetrexed based therapy (OR 2.46, p=0.017), and time to progression of greater than 12 months from first line therapy (OR 3.5 p=0.006). The progression free and OS was also related to time to progression of greater than 12 months after first line therapy (HR: 0.45; p<0.001 and HR: 0.54; p=0.005 respectively) and ECOG PS 0 (HR 0.67, p=0.022, HR: 0.43; p<0.001 respectively). In those previously exposed to pemetrexed, retreatment with a pemetrexed and platinum combination significantly reduced the risk-of-death than pemetrexed alone (HR: 0.11; p<0.001).
Rechallenge with Pemetrexed
A rechallenge with a pemetrexed-containing regimen could be considered in the second line if there was durable period of stable disease or response to treatment in the first line.
In an observational study by Ceresoli et al (2011) (26), 31 patients received pemetrexed based therapy as second line (18/31) or beyond second line treatment (13/31). Patients had at least 3 months of non-progressive disease after treatment with previous treatment with pemetrexed based regimens. The objective response rate was 19%, and a further 29% had stable disease. Whilst in the overall population, the median progression free survival (PFS) was 3.8 months and OS 10.5 months, patients with a first-line progression free survival of greater than 12 months had a longer median PFS after re-treatment (5.5 vs 2.5 months) when compared to patients with a shorter first line progression free survival.
These findings were similar to those found by Bearz et al (2012)(27) in a multi-institutional setting. Best response was stable disease in 50% of patients, partial response in 17% and reduction of pain was noted in 43%. Median time to progression on re-treatment was 5.1 months. There was no difference between time to progression of the group receiving pemetrexed alone or in combination with a platinum (4 vs. 5.7 months, p=0.77).
Other Single-Agent Chemotherapy Regimens
Single-agent chemotherapy regimens have been studied in Phase II studies with limited success. These would only be considered an option in patients who progress during first-line treatment with a pemetrexed based regimen, or where response to treatment is short, and no other effective treatment options are available.
Vinorelbine has been evaluated in small, non-comparative Phase II trials in the second line after previous treatment with a pemetrexed based regimen(28, 29). Reported response rates (partial at best) were 7-15%, with progression free survival of 2.3-2.5 months and OS of 4.5-6.2 months. In one study (28), factors such as ECOG performance status (PS) (0 vs. 1-2) HR 0.50; 95%CI: 0.3-0.8; p = 0.014) and PFS ≥ 6 months following first-line (FL) chemotherapy (HR(FL-PFS>6 months vs. <6 months) 0.50; 95%CI: 0.3-0.9; p = 0.031) were significantly associated with improved OS in multivariate analysis.
Gemcitabine alone has yielded disappointing response rates and overall median survival <5 months(30). A combination of both gemcitabine and vinorelbine has been studied in small, single-arm phase II studies (31, 32) with only modest efficacy and is not recommended as standard treatment.
Biologic Therapy
MPM cell lines express several angiogenic factors including members of the vascular endothelial growth factor (VEGF) family and its two receptors (VEGFR1 and VEGFR2). VEGF signalling can induce autocrine growth in malignant mesothelioma cells and have shown sensitivity to anti-VEGF agents in vitro (33, 34). Although there is strong rationale for inhibiting angiogenesis, few trials of anti-angiogenic agents in MPM have yielded positive results.
Bevacizumab is an anti-VEGF recombinant humanised IgG1 antibody derived from the murine monoclonal antibody A4.6.1. bevacizumab hampers the ability of VEGF to bind to VEGF receptors on the surface of endothelial or mesothelial cells and inhibit VEGF induced proliferation. The addition of bevacizumab to combination of cisplatin and pemetrexed has been trialled with statistically significant but small additional survival benefit (16.1 vs 18.8 months, HR 0.77 [0.62-0.95], p=0.0167) and expected added toxicities(35). Bevacizumab is not approved for use by the FDA. Therefore, due to significant out of pocket costs, it is not widely used and in many settings is not considered part of standard of care treatment.
Other antiangiogenesis agents however have proven less promising with both thalidomide and nintedanib failing to demonstrate clinical benefit.
Table 2. Biological Agents
Recommendation for Systemic Treatment in Developing Nations
The availability and accessibility of systemic treatments varies widely between and within developing nations. Therefore, where available, the first-line systemic therapy for MPM should be combination chemotherapy with cisplatin (or carboplatin) with pemetrexed. The World Health Organisation (WHO) Model List of Essential Medications (MLEM) (42) outlines the minimum medications needed for a basic health care system, listing the most efficacious, safe and cost effective pharmaceuticals for priority conditions, based on current and future public health relevance. This list includes both carboplatin and cisplatin for the treatment of non-small cell lung cancer. Although pemetrexed is not included, it is a reasonable expectation that its cost and availability will improve in future. The list also includes gemcitabine and vinorelbine for the treatment of non-small cell lung cancer, which are also second line options in MPM. Although the WHO MLEM does not specifically include drugs for the treatment of mesothelioma, it would suggest that these chemotherapy agents may be available in low-resource settings.
Where systemic therapies are not accessible, the recommended approach is best supportive care, focussing on palliation of symptoms and management of pleural effusions. Clinical trials are less available in developing nations and therefore experimental therapies or treatments with less evidence-base are not generally recommended. Biological agents (such as bevacizumab) and immunotherapy should be considered in centres with appropriate expertise and resources.
Radiation
Most patients with MPM present with advanced disease and associated symptoms. While MPM is generally considered to be radio-resistant, radiotherapy is a useful treatment modality in palliating symptoms of MPM, especially pain. The delivery of radiotherapy in MPM is technically challenging due to complex tumour shape, burden of disease, respiratory motion and surrounding radio-sensitive structures. Advanced conformal and intensity modulated techniques have been helpful in the safe delivery of appropriate doses of radiation.
For the role of radical radiotherapy as part of trimodality therapy see Section: Surgical Interventions and Palliative Procedures.
Palliative Radiotherapy
Radiation can be useful in the palliative management of MPM, particularly in pain management . Single centre studies of the use of radiotherapy for pain management caused by MPM have reported 47-65% of recipients experiencing benefit (43-48). No randomised trials or systemic reviews have demonstrated an survival advantage with the use of palliative radiotherapy (49, 50).
The prospective multicentre phase II SYSTEMS trial(43) assessed responses to pain at 1, 5 and 12 weeks following palliative radiotherapy (20Gy in 5 fractions) to painful chest lesions in patients with MPM. Of those assessable at the 5-week mark, 47% were reported to have improved pain. There were no improvements in symptoms other than pain (such as dyspnoea, fatigue, sweats, anxiety and depression) and minimal treatment-related toxicity. Another retrospective study by Jenkins et al(46) found that 57% of the studied cohort reported improvement in pain post-radiotherapy. In this study, response to treatment correlated with EORTC prognostic index (p=0.001), performance status (p=0.001) and histological subtype (0<0.001). A study by Bissett et al(48) suggested that wide-field radiotherapy (30Gy in 10 fractions) of the affected hemithorax was well tolerated, and most participants (68%) experienced symptom benefit after 1 month. The effect, however, was not long-lived with most (75%) patients reporting worsening pain at 3 months.
The optimal dose and fractionation is yet to be defined, however international guidelines(45) suggest standard palliative dosing regimens (such as single fraction of 8Gy) for MPM, although higher cumulative dosing and higher dose per fraction could be used to improve symptomatic response. There has been a prospective trial(51) of high dose palliative radiotherapy (45-60Gy using conformal and intensity-modulated techniques) which yielded significant excess toxicity without additional symptomatic benefit or survival. Researchers await the results from the SYSTEMS-2 trial(52), which is a randomised phase II trial comparing a standard regimen (20Gy in 5 fractions) with a dose-escalated regimen (36Gy in 6 fractions) for pain control in MPM. Currently, high dose radiotherapy with palliative intent remains outside of standard practice.
Radiotherapy to Prevent Instrumentation Tract Metastasis
Anecdotal concerns for patient with MPM regarding the potential for tumour seeding with instrumentation of the pleural space may result in a reluctance of clinicians to appropriately perform simple diagnostic or therapeutic procedures involving the pleura, particularly where radiotherapy is not available. It is important to note that the incidence of tract metastasis from large bore procedures in patients with MPM is low. Furthermore, the use of radiotherapy for preventing instrumentation tract metastases in MPM is not standard of care for those undergoing limited diagnostic or therapeutic procedures.
High quality phase III studies have shown no benefit in prophylactic radiotherapy in reducing incidence or improving symptom or QoL outcomes. Three small randomised trials had conflicting conclusions on the efficacy of prophylactic radiotherapy to prevent instrumentation tract metastases (53-55). These were followed by two randomised Phase III studies that showed no benefit of prophylactic radiotherapy in this setting.
The SMART trial(56) was multicentre phase III trial where patients were randomised to receive immediate or delayed radiotherapy (21Gy in 3 fractions) after large-bore pleural interventions such as video assisted thorascopic surgery (VATS), thoracoscopy or indwelling pleural catheter insertion. The overall incidence of tract metastasis was low and the early versus delayed strategy did not produce a statistically significant difference in incidence (9 vs 16%, OR 0.50 [CI 0.19-1.32], p=0.14). Notably, there was also no difference in symptom control, use of analgesia, survival or QoL. A large phase III trial (57) randomised patients to receive no prophylactic radiotherapy or 21Gy in 3 fractions within 42 days after instrumentation. There was no difference observed in the incidence of chest wall metastasis (3.2% vs 5.3%; OR 0.60 [0.17-1.86], p=0.44) between the groups. Careful clinical follow up and ad hoc radiotherapy for chest wall metastasis is recommended over prophylactic radiation.
Recommendations for Radiotherapy in Developing Nations
Radiotherapy can be a useful form of palliative treatment to reduce pain caused by MPM. There is no evidence to show survival benefit or reduction in respiratory symptoms such as dyspnoea or cough with palliative radiotherapy. There is no role for prophylactic radiotherapy to prevent tract metastases after instrumentation of the pleural space. In resource limited settings, radiotherapy may not be readily available or accessible and other available means of palliating symptoms should be explored including pharmacological and non-pharmacological strategies for pain management.
Surgical Interventions and Pallative Procedures
Few patients are eligible for radical surgery performed with curative intent due to extent of disease and functional status. Extra-pleural pneumonectomy (EPP) or extended pleurectomy/decortication (eP/D) have been performed in this setting to achieve maximal macroscopic resection. However, surgery alone has not shown adequate rates of disease control. A combined approach of surgery, chemotherapy and radiotherapy (Trimodality therapy aim to improve locoregional control and survival outcomes. As the majority of patients with MPM present with advanced, unresectable disease, in clinical practice, most surgical procedures are performed for the purposes of palliation and obtaining diagnosis. Partial pleurectomy/decortication is a palliative procedure performed in MPM to improve symptoms related to trapped lung. Pleurodesis is another palliative procedure performed to manage symptomatic, recurrent malignant effusions.
Table 3: IMIG and IASLC Uniform definitions of surgical techniques for MPM (2011) (58)
Extra Pleural Pneumonectomy (EPP)
EPP is an aggressive approach to achieve complete cytoreduction in MPM. Despite better rates of macroscopic clearance (58), EPP rarely results in long-term survival despite combination with chemotherapy and/or radiotherapy. Despite the more extensive surgery and potentially higher doses of adjuvant radiotherapy being able to be delivered after EPP (due to absence of ipsilateral lung), locoregional recurrence remain the most common site of treatment failure (59, 60). EPP is considered unsuitable for most patients with MPM due to higher perioperative mortality and post-operative morbidity. It is particularly unsuitable for those with poor prognostic factors (61) including cardiac risk factors, simultaneous N1 and N2 disease (62) and non-epithelioid histology.
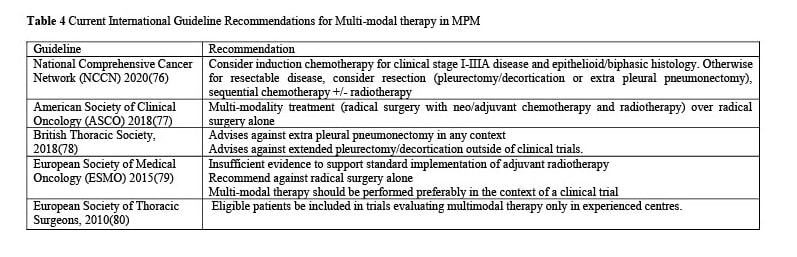
The 2018 British Thoracic Society guidelines advises against EPP in any context and eP/D outside of clinical trials. Meanwhile, the ASCO 2018 guidelines recommend radical surgery only in the context of multi-modality treatment (e.g. with neo/adjuvant chemotherapy and radiotherapy). Ultimately, studies of cancer registries in USA and Australia have shown low rates of EPP for MPM (6-8%)(63, 64). As there is no standardised approach to surgery for resectable MPM, radical surgery should only be considered in combination with chemotherapy and/or radiotherapy in highly specialised centres with experience and case-volume in addition to careful patient selection.
A systematic review by Cao et al (8), reviewed 58 studies including 2462 patients from 26 institutions. Median OS ranged from 9.4-27.5 months, with a median disease-free survival ranging between 7 to 19 months. Perioperative mortality rates varied widely from 0-11.8%, with significant perioperative morbidity rates (22-83%) and major morbidity rates (12.5-48%) noted. Only 3 studies looked at QoL, reporting a significant deterioration in QoL scores post-operatively, taking a further 3-6 months before improvement noted.
The 2011 MARS study(65) was undertaken as a prospective, randomised and controlled feasibility study to compare EPP or no-EPP in the context of multimodality therapy. 3 cycles of induction platinum-based therapy (investigator’s choice of mitomycin, vinorelbine and cisplatin, or cisplatin with gemcitabine, pemetrexed or vinorelbine) was given prior to randomisation. This study showed a significant detriment in survival outcomes for those patients undergoing EPP. A reduction in 12-month survival rates (52.2% [30.5-70.0] in the EPP arm vs. 73.1% in the no EPP arm [51.7-86.2]) was identified, and after adjustment for pre-specified prognostic factors, the hazard ratio for survival was 2.75 (1.21- 6.26, p=0.016). Median survival was 14.4 months vs. 19.5 months with no EPP. Investigators concluded that there was no survival advantage of EPP as part of multimodality therapy. Furthermore, as there were concerns regarding peri-operative safety (including a 10.5% 30-day mortality) and overall detriment to survival outcomes, the authors concluded a larger study could not be justified. These findings remain controversial as the MARS1 was criticised for being underpowered and the perioperative morbidity and mortality were higher than other studies reported in the literature. EPP remains utilised by some, and it is postulated that in a highly selective patient population with an experienced surgical team with good case-volume may be critical factors in obtaining optimal results.
Extended Pleurectomy/Decortication
Extended pleurectomy/decortication (extended P/D) is performed with curative intent where tumour is resected from the hemithorax including the diaphragm and/or pericardium (as required). The ipsilateral lung is spared. Many centres advocate eP/D over EPP due to lower rates of early complications and mortality, and comparable survival. A direct comparison between EPP and extended P/D is inherently difficult and to date, there have been no prospective randomised trial to compare the two surgical approaches.
A systematic review in 2013 by Cao et al(66) showed that extended P/D was associated with perioperative mortality ranging from 0-11%. Overall perioperative morbidity occurred in 20-43%. The reported median OS ranged between 11.5-31.7 months and disease-free survival between 7.2-16 months.
The largest descriptive case study to date is a retrospective of 663 consecutive patients who underwent EPP or P/D between 1990 and 2006 (67). The results suggested survival benefit in extended P/D, over EPP (p < .001). Multivariate analysis demonstrated a hazard ratio of 1.4 for EPP (p<0.001), after controlling for known factors that influenced survival on multivariate analysis, including AJCC stage (p < .001), epithelioid histology (P < .001), gender (P < .001) and multimodality therapy versus surgery alone (p < .001). The perioperative mortality rate was reported to be higher for EPP than for P/D (7% vs 4%). The authors however emphasised that the result of OS benefit is likely to be multifactorial and subject to patient selection bias. They concluded that resection technique should be based on individual comorbidities and the planned other multi-modal treatments.
Several other studies have reported on QoL and symptom outcomes and are also mostly in favour of extended P/D, mainly due to lower perioperative complications, better long term QoL, and longer survival post recurrence despite similar disease-free survival (68, 69). A randomised study (MARS2) is currently recruiting comparing extended P/D versus no extended P/D, with randomisation for surgical procedure occurring after 2 cycles of neoadjuvant cisplatin and pemetrexed chemotherapy. Study completion is expected in late 2020 and results by 2022. Extended P/D for MPM should only be performed in a carefully selected patient group, in high volume centres with surgeons of considerable experience or in the context of a clinical trial.
Trimodality therapy
In patients with resectable MPM who can be considered for EPP or extended P/D, a combined approach of surgery, chemotherapy and radiotherapy (Trimodality therapy) has been undertaken with the intent to improve locoregional control and survival outcomes. This approach is associated with high risk of treatment-related morbidity and mortality and is therefore recommended only to be performed in select patients in specialised centres with experience and expertise, preferably in the context of clinical trials.
International guidelines currently vary in their recommendations for multi-modal treatment for resectable mesothelioma. Best reported survival outcomes have been reported in series using multi-modal therapy, with median OS reported even up to 46.9 months(70-72). However, there have been no adequately powered randomised trials that have shown benefit of tri-modality therapy over chemotherapy or surgery alone(73). Systematic reviews of multimodality therapy have concluded that the evidence in favour of trimodality therapy over single-modality therapy (i.e. surgery or chemotherapy alone) is weak overall(73-75) and it is therefore paramount to carefully select candidates for trimodality therapy.
Table 3: IMIG and IASLC Uniform definitions of surgical techniques for MPM (2011) (58)
Extra Pleural Pneumonectomy (EPP)
EPP is an aggressive approach to achieve complete cytoreduction in MPM. Despite better rates of macroscopic clearance (58), EPP rarely results in long-term survival despite combination with chemotherapy and/or radiotherapy. Despite the more extensive surgery and potentially higher doses of adjuvant radiotherapy being able to be delivered after EPP (due to absence of ipsilateral lung), locoregional recurrence remain the most common site of treatment failure (59, 60). EPP is considered unsuitable for most patients with MPM due to higher perioperative mortality and post-operative morbidity. It is particularly unsuitable for those with poor prognostic factors (61) including cardiac risk factors, simultaneous N1 and N2 disease (62) and non-epithelioid histology.
The 2018 British Thoracic Society guidelines advises against EPP in any context and eP/D outside of clinical trials. Meanwhile, the ASCO 2018 guidelines recommend radical surgery only in the context of multi-modality treatment (e.g. with neo/adjuvant chemotherapy and radiotherapy). Ultimately, studies of cancer registries in USA and Australia have shown low rates of EPP for MPM (6-8%)(63, 64). As there is no standardised approach to surgery for resectable MPM, radical surgery should only be considered in combination with chemotherapy and/or radiotherapy in highly specialised centres with experience and case-volume in addition to careful patient selection.
A systematic review by Cao et al (8), reviewed 58 studies including 2462 patients from 26 institutions. Median OS ranged from 9.4-27.5 months, with a median disease-free survival ranging between 7 to 19 months. Perioperative mortality rates varied widely from 0-11.8%, with significant perioperative morbidity rates (22-83%) and major morbidity rates (12.5-48%) noted. Only 3 studies looked at QoL, reporting a significant deterioration in QoL scores post-operatively, taking a further 3-6 months before improvement noted.
The 2011 MARS study(65) was undertaken as a prospective, randomised and controlled feasibility study to compare EPP or no-EPP in the context of multimodality therapy. 3 cycles of induction platinum-based therapy (investigator’s choice of mitomycin, vinorelbine and cisplatin, or cisplatin with gemcitabine, pemetrexed or vinorelbine) was given prior to randomisation. This study showed a significant detriment in survival outcomes for those patients undergoing EPP. A reduction in 12-month survival rates (52.2% [30.5-70.0] in the EPP arm vs. 73.1% in the no EPP arm [51.7-86.2]) was identified, and after adjustment for pre-specified prognostic factors, the hazard ratio for survival was 2.75 (1.21- 6.26, p=0.016). Median survival was 14.4 months vs. 19.5 months with no EPP. Investigators concluded that there was no survival advantage of EPP as part of multimodality therapy. Furthermore, as there were concerns regarding peri-operative safety (including a 10.5% 30-day mortality) and overall detriment to survival outcomes, the authors concluded a larger study could not be justified. These findings remain controversial as the MARS1 was criticised for being underpowered and the perioperative morbidity and mortality were higher than other studies reported in the literature. EPP remains utilised by some, and it is postulated that in a highly selective patient population with an experienced surgical team with good case-volume may be critical factors in obtaining optimal results.
Extended Pleurectomy/Decortication
Extended pleurectomy/decortication (extended P/D) is performed with curative intent where tumour is resected from the hemithorax including the diaphragm and/or pericardium (as required). The ipsilateral lung is spared. Many centres advocate eP/D over EPP due to lower rates of early complications and mortality, and comparable survival. A direct comparison between EPP and extended P/D is inherently difficult and to date, there have been no prospective randomised trial to compare the two surgical approaches.
A systematic review in 2013 by Cao et al(66) showed that extended P/D was associated with perioperative mortality ranging from 0-11%. Overall perioperative morbidity occurred in 20-43%. The reported median OS ranged between 11.5-31.7 months and disease-free survival between 7.2-16 months.
The largest descriptive case study to date is a retrospective of 663 consecutive patients who underwent EPP or P/D between 1990 and 2006 (67). The results suggested survival benefit in extended P/D, over EPP (p < .001). Multivariate analysis demonstrated a hazard ratio of 1.4 for EPP (p<0.001), after controlling for known factors that influenced survival on multivariate analysis, including AJCC stage (p < .001), epithelioid histology (P < .001), gender (P < .001) and multimodality therapy versus surgery alone (p < .001). The perioperative mortality rate was reported to be higher for EPP than for P/D (7% vs 4%). The authors however emphasised that the result of OS benefit is likely to be multifactorial and subject to patient selection bias. They concluded that resection technique should be based on individual comorbidities and the planned other multi-modal treatments.
Several other studies have reported on QoL and symptom outcomes and are also mostly in favour of extended P/D, mainly due to lower perioperative complications, better long term QoL, and longer survival post recurrence despite similar disease-free survival (68, 69). A randomised study (MARS2) is currently recruiting comparing extended P/D versus no extended P/D, with randomisation for surgical procedure occurring after 2 cycles of neoadjuvant cisplatin and pemetrexed chemotherapy. Study completion is expected in late 2020 and results by 2022. Extended P/D for MPM should only be performed in a carefully selected patient group, in high volume centres with surgeons of considerable experience or in the context of a clinical trial.
Trimodality therapy
In patients with resectable MPM who can be considered for EPP or extended P/D, a combined approach of surgery, chemotherapy and radiotherapy (Trimodality therapy) has been undertaken with the intent to improve locoregional control and survival outcomes. This approach is associated with high risk of treatment-related morbidity and mortality and is therefore recommended only to be performed in select patients in specialised centres with experience and expertise, preferably in the context of clinical trials.
International guidelines currently vary in their recommendations for multi-modal treatment for resectable mesothelioma. Best reported survival outcomes have been reported in series using multi-modal therapy, with median OS reported even up to 46.9 months(70-72). However, there have been no adequately powered randomised trials that have shown benefit of tri-modality therapy over chemotherapy or surgery alone(73). Systematic reviews of multimodality therapy have concluded that the evidence in favour of trimodality therapy over single-modality therapy (i.e. surgery or chemotherapy alone) is weak overall(73-75) and it is therefore paramount to carefully select candidates for trimodality therapy.
Table 4. Current International Guideline Recommendations for Multi-modal therapy in MPM
As previously discussed, the excess morbidity and mortality conferred by EPP appears to be a limiting factor for trimodality therapy, with a large proportion (50-58%) of patients being unable to complete all treatment modalities largely due to surgical complications or progressive disease during treatment (81, 82). A retrospective review by DePerrot et al(81) found only half those who attempted trimodality therapy completed the full course of treatment. All patients received at least 3 cycles of induction cisplatin-based chemotherapy. One quarter (25%) did not proceed to surgery due to unresectability or progression of disease. Another 25% did not proceed to radiotherapy due to post-operative complications, poor functional status after surgery or further progressive disease. There was a perioperative mortality rate of 6.7%. The median OS was 14 months, with a 5-year survival rate of 10%. Multivariate analysis demonstrated that N2 disease was the most significant prognostic marker of worse outcome.
Treatment related complications and morbidity was also a major limiting factor identified in the EORTC Phase II trial (82) which aimed to administer trimodality therapy to 57 patients with resectable MPM. Less than half the studied population (42.1%) were able to complete the full course of treatment within prespecified timeframes. The median OS in this group was 18.4 months. Chemotherapy has been increasingly utilised in trials with or without cancer directed surgery for MPM(63) – likely due to the landmark trial in 2003 by Vogelzang et al(1), which demonstrated survival benefit with the use of combination platinum based treatment in unresectable MPM.
A systematic review (74) identified eight studies that utilised chemotherapy in the neoadjuvant setting and a further 8 that used adjuvant chemotherapy as part of trimodality treatment of MPM. The outcomes were difficult to compare given that the chemotherapy regimen, patient selection, follow up periods and reporting of survival outcomes varied between the trials. Overall, studies of adjuvant chemotherapy as part of trimodality therapy reported median OS periods of 19-24 months and median disease free survival of 10-15 months(74).
Trials involving neoadjuvant chemotherapy were similar in outcomes, with median OS 16.8-22.5 months and disease free survival of 10.1-16.3 months(74). Four of the more recent prospective phase II trials(82-85) using neoadjuvant chemotherapy, EPP and adjuvant radiotherapy showed that majority of patients (55-71%) completed trimodality treatment on an intention-to-treat analysis, and the perioperative mortality was 0-5%.
Complications from adjuvant radiotherapy is a limiting factor in delivering trimodality therapy. As the pleura has a large surface area, the volumes required for conventional radiotherapy is high. When radiotherapy is utilised after lung-sparing radical surgery (i.e. extended pleurectomy and decortication, rather than EPP), there is a risk of radiation-induced pneumonitis to the ipsilateral lung. Effective adjuvant radiotherapy aims to improve locoregional disease control with adequate delivery of radiation dose, while minimising excess radiation pneumonitis.
A phase II trial of adjuvant hemi-thoracic RT (54 Gy) following EPP demonstrated high rates of local control, with only two isolated loco-regional failures in 54 patients and a median survival of 17 months(86). The SAKK 17/04 trial (87) was a phase II randomised study that compared radical radiotherapy or no radiotherapy in patients who achieved complete macroscopic resection after induction platinum-based chemotherapy and EPP. Complete macroscopic resection was achieved in 64% of the study cohort, however only 35% of the cohort were randomised for radiotherapy, mainly due to patient decision not to participate. Most patients completed radiotherapy (median dose of 55.9 Gy) and there was one death from radiation pneumonitis. The authors found no survival benefit of additional hemithoracic radiotherapy despite better locoregional control. Overall, the authors concluded routine hemithoracic radiotherapy could not be recommended after induction chemotherapy and surgery.
Intensity modulated conformational techniques have been used to allow more effective sparing of adjacent structures and higher dosimetric control. A potential disadvantage of intensity modulated radiotherapy (IMRT) after EPP is the dose of radiation delivered to the contralateral lung and the risk of pneumonitis(88). Pulmonary toxicity is dependent on both lung volumes and the radiation dose. IMRT is also particularly useful after extended P/D as patients have both lungs in situ.
A single arm Phase II study of hemithoracic IMRT(89) after induction chemotherapy and (if feasible) extended P/D showed median progression-free survival of 12.4 months and OS of 23.7 months. The two-year OS was 59 percent in patients with resectable tumours and 25 percent in patients with unresectable tumours. A follow-up retrospective study (90) suggested that outcome was better with pleural IMRT, compared to conventional techniques.
While we await the results of the MARS2 study assessing multimodality therapy in the context of the extended pleurectomy and decortication, it is important to highlight that any such aggressive treatment approach should be limited only to high volume centres with appropriate surgical and post-operative expertise and resources, and as such should be considered inappropriate in the majority of developing nations.
Palliative Pleurectomy and Decortication
As most patients with MPM present with advanced, unresectable disease, most surgical procedures are undertaken with palliative intent to improve symptoms related to malignant effusions or tumour burden. Partial (debulking) pleurectomy with or without decortication is utilised for patients with MPM to improve symptom burden and improve QoL, particularly in those patients where visceral pleural disease limits lung expansion. A systematic review by Cao et al (2013)(66) showed that perioperative mortality ranged 0-7.1% for palliative P/D, with morbidity ranging 13-48% and marked heterogeneity in median OS (8.3-26 months) between studies. These findings are not dissimilar to those assessing partial pleurectomy with regard to mortality (0-7.8%), morbidity (14-20%) and OS (7.1-14 months).
To date, no clear survival benefit has been demonstrated for these procedures, however symptomatic benefits in dyspnoea and pain have been seen. A prospective cohort study (91) of 116 patients receiving partial pleurectomy (n=17) and decortication (n=34), reported a 30-day post-operative mortality rate of 7.8%, and significant morbidity (e.g. persistent air leak more than 7 days) was noted in 15% of the open decortication group. The type of procedure did not influence survival and symptom benefits in dyspnoea and pain were seen at 6 weeks and 3 months post procedure – however mortality from progressive disease outweighed the symptomatic benefits after this point. Multivariate analysis identified a select group of patients (epithelioid histology, no weight loss) who were more likely to retain symptomatic control with palliative surgery (p<0.01). We await the results of the MESO TRAP trial, which is an ongoing phase III study comparing VATS-partial pleurectomy/decortication vs. indwelling pleural catheter in patients with trapped lung due to MPM.
Pleuroedesis and Indwelling Pleural Catheters
Most (95%) patients with MPM develop pleural effusions which cause decrement in QoL without intervention. Pleurodesis is a palliative procedure where permanent pleural apposition is achieved through chemical or physical means – commonly through instillation of talc. Talc pleurodesis is a conventionally recommended intervention to control symptomatic effusions, mainly based on extrapolated data from studies in malignant pleural effusions with metastatic carcinomas. It is generally considered a safe procedure despite procedure related complications (mainly pain and fever resulting from intense pleural inflammation) and low reported rates of infective complications (3%) (92) or fatal acute respiratory distress syndrome (RDS) (93). Talc is an inexpensive substance that is available worldwide including in developing nations(94).
The optimal method of pleurodesis remains uncertain. Surgical pleurodesis is one method of creating pleural apposition through mechanical abrasion or parietal pleurectomy via thoracotomy or VATS has replaced open thoracotomy as the first line surgical procedure of choice in many developed nations(95), in developing nations with limited access to VATS, a traditional open surgical approach may be utilised – however with expected increased risk of morbidity.
An Australian registry based retrospective study of 390 patients between 2004-2009 found 165 (42.3%) patients had pleurodesis (surgical n=78; bedside talc n=86, bleomycin n=1)(92). Most surgical pleurodesis was performed during VATS and all involved talc poudrage. A completely successful pleurodesis (no further fluid accumulation) was achieved in 29.7% and partial success in 38.8%. No differences were seen in treatment success rates between surgical and bedside pleurodesis. Surgical pleurodesis was more often performed in younger patients (median age 67.1 vs. 72.3 years, p<0.01) and at time of diagnostic procedures, compared to bedside talc instillations.
Median survival was longer in those who underwent pleurodesis (443 vs. 193 days; p= 0.002), with better outcomes in those with completely successful pleurodesis. These findings are similar to prospective randomised trials assessing surgical and bedside pleurodesis for malignant effusions have found no advantage of VATS talc poudrage over bedside pleurodesis (93).
MESO-VATS(96) is the only RCT comparing VAT partial pleurectomy (VAT-PP) and talc pleurodesis in patents with MPM and pleural effusion. Both interventions provided similar, significant reduction in pleural effusion (70% VATS vs. 77% talc), without difference in overall QoL outcomes. Survival was similar in both arms at 12 months. Overall, the less invasive approach would beecommended to control pleural effusion, especially as a palliative procedure.
An alternative method of managing recurrent pleural effusions is an indwelling pleural catheter (IPC). IPCs are silicon tubes tunnelled and secured subcutaneously, ending in a one-way valve. It allows ambulatory drainage of pleural effusions to provide symptom relief without needing to create pleural apposition. IPCs can be more useful, particularly in those patients with visceral pleural involvement from MPM where pleural apposition may not be possible due to limited lung re-expansion. Other benefits include reduced length of stay (LOS) and lower rates of subsequent thoracocentesis (97).
A systematic review(98) of RCTs of talc pleurodesis in malignant pleural effusion found IPCs were associated with shorter procedure-related hospital stay and lower risks of further ipsilateral pleural interventions when compared with chemical pleurodesis. Conversely, IPCs were associated with a higher risk of cellulitis. There were no differences in control of dyspnoea or survival. The drainage regimen should be symptom-guided, with no difference between daily drainage vs. symptom guided drainage in providing symptom relief from dyspnoea in a randomised trial (AMPLE-2)(99).
There are multiple potential issues with IPC including additional cost and expertise required for tunnelled placement. Where IPCs are not accessible, repeated thoracocentesis would be a reasonable alternative. IPC s are also associated with infections – however reported rates of empyema and cellulitis are low (2.8% and 3.4% respectively)(100). Immunosuppression from chemotherapy did not increase pleural infection rates from IPC(101, 102). There is also risk of catheter related pain, symptomatic loculations, catheter blockage and fracture and protein depletion (103). Catheter tract metastasis is uncommon and recommended to be treated ad hoc with radiotherapy if accessible.
Recommendations for Surgical Interventions and Procedures in Developing Nations
Although the appropriate method of surgical management of mesothelioma remains controversial, trimodality therapy including EPP and eP/D should only be undertaken in specialist centres with expertise and resources, and ideally within a clinical trial setting. It is considered inappropriate for extensive operative management including EPP and eP/D to be considered outside of high volume, experienced centres with appropriate post-operative support including the availability of intensive care units. It is therefore not recommended this be undertaken in resource limited settings.
We recognise there is wide variability between and within developing nations in the availability of palliative surgical interventions for MPM such as partial pleurectomy and decortication, VATS pleurodesis or IPCs. The decision regarding appropriate modality is highly dependent upon the resources available and patient access to these. As such, pleural drainage (either intermittently through thoracocentesis, with or without the use of talc pleurodesis) remains the minimum standard of care globally including in low resource nations.
Palliative Care
Palliative care is the active management of patients with life-limiting, progressive, malignant, and non-malignant illnesses. This approach aims to improve the QoL of patients and their carers/families through prevention and relief of suffering, through assessment and treatment of physical symptoms as well as psychosocial and spiritual issues. For MPM, palliative care is applicable at any time between diagnosis and death and is provided concurrently with anti-cancer therapies with the aim of enhancing QoL, comfort and preserving dignity. The palliative management of symptoms are described further in Section 4: Patient Support.
Table 5: The World Health Organisation Definition of Palliative Care (104)
Effective palliative care is necessary in the management of patients with mesothelioma as an aggressive malignancy with high symptom burden, limited treatment options and short prognosis. In low resource settings, it is likely most palliative care will be delivered by community health care workers, rather than a specialist palliative care service. The 2018 Lancet Commission on Palliative Care and Pain Relief (105) describes significant inequity across the globe in relation to access to palliative care and opioids.
Globally, the need for palliative care is large and continues to grow. There are existing barriers to accessing opioids in low- and middle-income countries (LMIC), including lack of policy and investments into palliative care in addition to regulatory hurdles due to fear of non-medical use of opioids and side-effects. The Lancet Commission report also outlines an “essential package” of essential human resources, equipment and medications that form the basic inputs required for the safe and effective provision of essential palliative care in a primary care setting. The listed medications are also present on the WHO List of essential medicines and only includes off-patent formulations obtainable at low cost. The essential package also recommends that frugal innovation to provide for necessary equipment and empowerment, training and supervision of community health-care workers is an essential part of effective and safe delivery of palliative care and analgesia in low-resource settings.
Pain
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or describe in terms of such damage(106). Pain in MPM can present with mixed nociceptive and neuropathic features owing from direct infiltration of soft tissue, bone and intercostal nerves(107). Pain for patients with MPM can therefore be complex and challenging, requiring a multi-faceted approach for effective management. In the Lancet Commission’s essential package for palliative care, five of the listed essential medications are commonly used in the management of cancer pain (morphine, amitriptyline, ibuprofen, dexamethasone, and paracetamol). The WHO’s 1986 Analgesic Ladder for Cancer Pain Relief (108) describes a 3-step approach to provide adequate pain relief for cancer patients, attempting to match the type of analgesia to the intensity of pain.
Additional recommendations supporting the implementation of the WHO analgesic ladder in cancer pain recommend that oral analgesia should be prescribed where possible to grant patients more control over pain management. Analgesia should be given with appropriate guidance and education and be given at regular intervals “by the clock” according to expected pharmacokinetics. If available, slow, or modified release formulations of opioids can be given regularly with short-acting formulations for ‘break-through’ pain. There are no standard doses for opioids for the treatment of cancer pain. Analgesia should be titrated and adapted to each individual patient and their pain intensity (See also Section: Patient Support). In the multi-center European Pharmacogenetic Opioid Study (EPOS) study(109), the mean total daily oral morphine equipotent dose for patients with mesothelioma ranged from 30.0 – 960.0mg (median 160mg). Half (50%) of the mesothelioma cohort were also taking systemic steroids. Only a minority (18%) of patients achieved complete control of pain. Where accessible, radiotherapy should additionally be considered for control of pain related to MPM. The SYSTEMS study (2015) demonstrated a clinically significant improvement in pain with radiotherapy (20Gy in 5 fractions) assessed at Week 5.
Furthermore, when other simpler measures have failed and where available, interventional procedures can also be considered for local control of pain. This may include peripheral (e.g., intercostal) nerve block or neurolysis. This involves injection of a local anaesthetic or ablative substance (e.g., alcohol) to induce loss of sensation in the distal neural distribution with analgesic intent. One series of intercostal blocks in patients with advanced cancer and painful rib metastases showed 56% described reduced analgesic requirements post-procedure (110).
High cervical cordotomy has also been described for palliation of pain in mesothelioma. This involves intentional damage to the ascending pathways of the spinothalamic tract in the antero-lateral spinal cord. This aims to reduce afferent, unilateral pain sensation below the level of C4. Although a systemic review(111) has shown effective, mostly short-term relief of pain when used in patients with MPM, the evidence base is small and carries potentially significant procedural risk (headache, mirror pain, motor weakness, respiratory dysfunction). This should only be undertaken in experienced tertiary centres.
Other palliative therapies, such as chemotherapy, see text on Systemic Therapies.
Dyspnoea/Cough
Dyspnoea and cough from MPM can be multifactorial, distressing, and difficult to control. Management is aimed at identifying the underlying causes, treating what is reversible, whilst also actively reducing the symptom burden with appropriate pharmacological and non-pharmacological interventions and strategies.
Appropriate examination and investigations should be undertaken to determine the underlying causes as dyspnoea and cough can be related to both malignant (e.g., pleural effusion, trapped lung) and non-malignant causes (e.g. infection, chronic obstructive pulmonary disease (COPD), heart failure, anaemia and anxiety). Recurrent malignant pleural effusion remains a major cause of dyspnoea in patients with MPM. Please refer to Chapter 3.4 for discussion of pleurodesis and indwelling pleural catheters.
A hand-held fan is a portable and cheap device which has been shown to alleviate chronic breathlessness(112). Although the mechanisms are not fully understood, airflow has been postulated to influence afferent sources for respiratory sensation. Several trials(113-115) have found significant reduction in severity of dyspnoea from short-term use of a hand-held fan in patients with chronic breathlessness. In addition, patient education about breathlessness in addition to anxiety reduction training (such as intentional diaphragmatic breathing and relaxation techniques) can be helpful in managing the fear/anxiety associated with dyspnoea.
Hypoxia is an end consequence of many conditions associated with MPM causing dyspnoea. Oxygen is listed as an essential device in the Lancet Commission’s Essential Package for Palliative Care and should be provided where accessible to alleviate dyspnoea. In those who are mildly hypoxic and without access to domiciliary oxygen, room air administered via nasal cannula at 2L/min can also be a potential alternative to palliate symptoms. A double-blind, randomised study of 239 participants with life-limiting illness, refractory dyspnoea and PaO2 > 7.3 were randomly assigned to receive oxygen or room air at 2L/min for 7 days. There was no additional benefit of oxygen in this setting(116).
Opioids have also been used in populations with life limiting disease and refractory dyspnoea with good effect. A systematic review and meta-analysis(117) showed a statistically significant, positive effect of opioids on the sensation of breathlessness (p=0.0008). Meta-regression of subgroups showed a greater effect for the oral or parenteral route compared to nebulised opioids. Opioids have also been used with good effect in patients with terminal lung cancer with refractory dyspnoea at rest(115).
Benzodiazepines are also frequently used as an adjunctive therapy to opioids in patients with refractory dyspnoea. A Cochrane review(118) found there was limited evidence for or against benzodiazepine use in refractory malignant or non-malignant dyspnoea, and supports its use if other first line treatments have failed. Cough is also a common symptom in patients with MPM. Chronic cough resulting from disease progression are managed with opioid based anti-tussive (including morphine, codeine) (119) however there are limited high-quality studies investigating this.
Recommendation for Palliative Care in Low Resource Settings
Effective palliative care is essential in the management of MPM. Pain, dyspnoea, and cough are the most common physical symptoms caused by MPM that can be managed through a combination of non-pharmacological and pharmacological interventions. Despite barriers to access specialist palliative care services and appropriate pharmaceuticals and equipment in low-resource settings, international guidelines suggest community health care workers can be trained, empowered, and supervised to delivery safe, appropriate and effective palliative care.
Novel Treatment Options
Newer therapy options have garnered much interest. Recent developments have established the role of immune checkpoint inhibitors (ICI) in the treatment of MPM Where resources allow, the use of ICI should be considered, particularly in those with a sarcomatoid subtype of MPM. ICI however remain costly and are inaccessible for many.
The WHO MLEM added ICI in 2019 for the treatment of metastatic melanoma (nivolumab or alternatively pembrolizumab). The cost of medications is only one of many challenges in the treatment of cancer patients in developing nations, which may include systemic issues such as limited numbers of trained health professionals and late presentations with cancer. Other novel treatment strategies such as photodynamic therapy, gene therapy, CAR-T and tumour treatment fields remain only available in trial settings.
Immunotherapy
Studies of single-agent ICI in the second-line treatment of MPM has not demonstrated significant clinical benefit in trial settings. PD-(L)1 inhibitors have shown response rates between 10-29% in Phase II trials(120-127), with a wide range reported in progression free survival and OS. Survival benefit over standard second-line options has not been demonstrated in randomised Phase III trials. For example, he PROMISE-Meso(128) trial failed to demonstrate superior survival benefit of pembrolizumab (PD-1 inhibitor) over second line chemotherapy (gemcitabine or vinorelbine). The phase IIb DETERMINE trial(126) also did not show survival advantage of tremelimumab (CTLA-4 inhibitor) over placebo in the second or third line.
The combination of CTLA and PD-1 blockade has recently emerged as a new first line treatment option in patients with MPM. The CHECKMATE-743(129) trial is a large phase III trial which randomised 605 patients to pemetrexed with cis/carboplatin or combination immunotherapy (nivolumab and ipilimumab). Interim analysis presented in August 2020 has demonstrated OS advantage of dual immunotherapy over standard cisplatin and pemetrexed chemotherapy (18.1 versus 14.1 months, HR 0.74 [0.60-0.91], p=0.002). Benefit was particularly seen in the non-epithelioid subgroup and in those with PDL1 expression 1%.
Other trials combining standard chemotherapy with immunotherapy with/out anti-angiogenic agents are in progress.
Recommendation for New(er) Treatments in Low Resource Settings
• In low-resource settings, the availability of newer treatments and trials may be limited. If accessible, ICI could be considered in the palliative treatment of MPM.
• Other novel treatment strategies such as photodynamic therapy, gene therapy, CAR-T and tumour treatment fields remain only available in trial settings.
Gene Therapy
Gene therapy involves the transfer of genetic material (such as complementary DNA, genes, RNA or oligonucleotides) into cancer cells via engineered viruses. Several different approaches have been studied in MPM including delivery of cell ‘suicide’ genes, tumour suppressor genes and genes to modulate immune response. Gene therapy is mostly studied in pre-clinical or phase I settings.
For further reading see References 143-150
Photodynamic Therapy
Intra-cavitary photodynamic therapy (PDT) has been investigated as an adjuvant local therapy in surgically resected mesothelioma. An intravenous photo-sensitiser is administered prior to planned EPP or pleurectomy/decortication. After maximal surgical resection, the pleural cavity is treated with laser calibrated to a particular wavelength (nm) and light dose (J/cm2) Although early studies were promising, two small, phase III studies have shown mixed results. PDT has not entered wider use and is recommended (135) only to be utilised in experienced cancer centres, preferably in the setting of a clinical trial.
For further reading see References 151-160
CAR-T Cells
One investigative approach of harnessing the immune system in treating cancer is the administration of tumour antigen-targeted T cells that are engineered to directly target tumour cells. A chimeric antigen receptor (CAR) typically contains an extra-cellular, antigen-recognition domain, a transmembrane domain and an intracellular domain that contain three immune receptor tyrosine-based activation motifs. The CAR is transfected into autologous T-cells via mRNA or viral transduction(136, 137). CAR-T cells have been used in haematological malignancies with promising results, however, face many challenges in solid tumours. In MPM, several potential tumour-antigen targets have been identified such as MSLN, WT-1, FAP and antigens of the ErbB family. As a therapeutic strategy for MPM, CAR-T cells are only available in pre-clinical/early clinical trials.
For further reading see References 161-166
Tumour Treating Fields
Tumour Treating Fields (TTF) are a non-invasive, regional treatment for solid tumours(138) which involves the delivery of low-intensity alternating electric fields to the region of known tumour and has been studied as an adjuvant treatment for brain tumours(139). TTF have been shown to disrupt the assembly of the mitotic spindle essential for mitosis and also to change cellular membrane structures in glioblastoma cell models, potentially increasing permeability to chemotherapy(140, 141). TTF have recently been Food and Drug Administration (FDA) approved for the treatment of mesothelioma based on a single-arm, phase II study(142) which applied TTF during standard first line chemotherapy with cis/carboplatin and pemetrexed. This study had encouraging survival results and no increase in systemic toxicity. This treatment modality requires further investigation in larger trials.
For further reading see References 167-170
References
Vogelzang NJ, Rusthoven JJ, Symanowski J, Denham C, Kaukel E, Ruffie P, et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol. 2003;21(14):2636-44. doi: http://dx.doi.org/10.1200/JCO.2003.11.136 PMID: 12860938
Ong ST, Vogelzang NJ. Chemotherapy in malignant pleural mesothelioma. A review. J Clin Oncol. 1996;14(3):1007-17. doi: http://dx.doi.org/ 10.3978/j.issn.2225-319X.2012.10.05 PMID: 23977545
Hollen PJ, Gralla RJ, Liepa AM, Symanowski JT, Rusthoven JJ. Measuring quality of life in patients with pleural mesothelioma using a modified version of the Lung Cancer Symptom Scale (LCSS): psychometric properties of the LCSS-Meso. Support Care Cancer. 2006;14(1):11-21. doi: http://dx.doi.org/10.1007/s00520-005-0837-0 PMID: 15999264
Gralla RJ HP, Am L, Liepa AM, et al. Improving quality of life in patients with malignant pleural mesothelioma: Results of the randomized pemetrexed and cisplatin vs. cisplatin trial using the LCSS-meso instrument. Proc Am Soc Clin Oncol. 2003;22(Abstr 2496).
Symanowski JT RJ, Nguyen B, Ruffie P, Moro-Sibilot D, Dabouis G et al. Multiple regression analysis of prognostic variables for survival from the phase III study of pemetrexed + cisplatin vs. cisplatin in malignant pleural mesothelioma. Proc Am Soc Clin Oncol. 2003;22(Abstr 2602).
Santoro A, O’Brien ME, Stahel RA, Nackaerts K, Baas P, Karthaus M, et al. Pemetrexed plus cisplatin or pemetrexed plus carboplatin for chemonaive patients with malignant pleural mesothelioma: results of the International Expanded Access Program. J Thorac Oncol. 2008;3(7):756-63. doi: http://dx.doi.org/ 10.1097/JTO.0b013e31817c73d6
Castagneto B, Botta M, Aitini E, Spigno F, Degiovanni D, Alabiso O, et al. Phase II study of pemetrexed in combination with carboplatin in patients with malignant pleural mesothelioma (MPM). Ann Oncol. 2008;19(2):370-3. doi: http://dx.doi.org/ 10.1093/annonc/mdm501 PMID: 18156144
Ceresoli CL, Zucali PA, Favaretto AG, Grossi F, Bidoli P, Del Conte G, et al. Phase II study of pemetrexed plus carboplatin in malignant pleural mesothelioma. J Clin Oncol. 2006;24(9):1443-8. doi: http://dx.doi.org/10.1200/JCO.2005.04.3190 PMID:16549838
Katirtzoglou N, Gkiozos I, Makrilia N, Tsaroucha E, Rapti A, Stratakos G, et al. Carboplatin plus pemetrexed as first-line treatment of patients with malignant pleural mesothelioma: a phase II study. Clin Lung Cancer. 2010;11(1):30-5. doi: http://dx.doi.org/10.3816/CLC.2010.n.005 PMID: 20085865
Ceresoli GL, Castagneto B, Zucali PA, Favaretto A, Mencoboni M, Grossi F, et al. Pemetrexed plus carboplatin in elderly patients with malignant pleural mesothelioma: combined analysis of two phase II trials. Br J Cancer. 2008;99(1):51-6. doi: http://dx.doi.org/10.1038/sj.bjc.6604442 PMID: 18542071
van den Bogaert DP PE, van Wijhe G, et al. Pemetrexed maintenance therapy in patients with malignant pleural mesothelioma. J Thorac Oncol. 2006;1:25-30. doi: http://dx.doi.org/10.1016/S1556-0864(15)31509-4 PMID: 17409823
Dudek AZ, Wang X, Gu L, Duong S, Stinchcombe TE, Kratzke R, et al. Randomized Study of Maintenance Pemetrexed Versus Observation for Treatment of Malignant Pleural Mesothelioma: CALGB 30901. Clin Lung Cancer. 2020;21(6):553-61 e1. doi: http://dx.doi.org/10.1016/j.cllc.2020.06.025
O’Brien ME, Watkins D, Ryan C, Priest K, Corbishley C, Norton A, et al. A randomised trial in malignant mesothelioma (M) of early (E) versus delayed (D) chemotherapy in symptomatically stable patients: the MED trial. Ann Oncol. 2006;17(2):270-5. doi: http://dx.doi.org/10.1093/annonc/mdj073 PMID:16317014
van Meerbeeck JP, Gaafar R, Manegold C, Van Klaveren RJ, Van Marck EA, Vincent M, et al. Randomized phase III study of cisplatin with or without raltitrexed in patients with malignant pleural mesothelioma: an intergroup study of the European Organisation for Research and Treatment of Cancer Lung Cancer Group and the National Cancer Institute of Canada. J Clin Oncol. 2005;23(28):6881-9. doi: http://dx.doi.org/10.1200/JCO.20005.14.589 PMID: 16192580
Nowak AK, Byrne MJ, Williamson R, Ryan G, Segal A, Fielding D, et al. A multicentre phase II study of cisplatin and gemcitabine for malignant mesothelioma. Br J Cancer. 2002;87(5):491-6. doi: http://dx.doi.org/ 10.1038/sj.bjc.6600505 PMID: 12189542
Byrne MJ, Davidson JA, Musk AW, Dewar J, van Hazel G, Buck M, et al. Cisplatin and gemcitabine treatment for malignant mesothelioma: a phase II study. J Clin Oncol. 1999;17(1):25-30. doi: http://dx.doi.org/10.1200/JCO.1999.17.1.25 PMID: 10458214
van Haarst JM, Baas P, Manegold C, Schouwink JH, Burgers JA, de Bruin HG, et al. Multicentre phase II study of gemcitabine and cisplatin in malignant pleural mesothelioma. Br J Cancer. 2002;86(3):342-5. doi: http://dx.doi.org/10.1038/sj.bjc.6600118 PMID:11875695
Castagneto B, Zai S, Dongiovanni D, Muzio A, Bretti S, Numico G, et al. Cisplatin and gemcitabine in malignant pleural mesothelioma: a phase II study. Am J Clin Oncol. 2005;28(3):223-6. doi: http://dx.doi.org/10.1097/01.coc.0000144852.75613.56 PMID: 15923792
Kalmadi SR, Rankin C, Kraut MJ, Jacobs AD, Petrylak DP, Adelstein DJ, et al. Gemcitabine and cisplatin in unresectable malignant mesothelioma of the pleura: a phase II study of the Southwest Oncology Group (SWOG 9810). Lung Cancer. 2008;60(2):259-63. doi: http://dx.doi.org/10.1016/j.lungcan.2007.09.018. PMID: 18006112
Favaretto AG, Aversa SM, Paccagnella A, Manzini Vde P, Palmisano V, Oniga F, et al. Gemcitabine combined with carboplatin in patients with malignant pleural mesothelioma: a multicentric phase II study. Cancer. 2003;97(11):2791-7. doi: http://dx.doi.org/10.1002/cncr.11405 PMID: 12767092
Favaretto AG, Aversa SML, Paccagnella A, Manzini VDP, Palmisano V, Oniga F, et al. Gemcitabine combined with carboplatin in patients with malignant pleural mesothelioma. Cancer. 2003;97:2791-7. doi: http://dx.doi.org/10.1002/cncr.11405 PMID: 12767092
Muers MF, Stephens RJ, , Fisher P, Darlison L, Higgs CM LowryE, et al. Active symptom control with or without chemotherapy in the treatment of patients with malignant pleural mesothelioma (MS01): a multicentre randomised trial. Lancet. 2008 371(9625):1685–94. doi: http://dx.doi.org/10.1016/S0140-6736(08)60727-8 PMID: 18486741
Janne PA, Wozniak AJ, Belani CP, Keohan ML, Ross HJ, Polikoff JA, et al. Pemetrexed alone or in combination with cisplatin in previously treated malignant pleural mesothelioma: outcomes from a phase IIIB expanded access program. J Thorac Oncol. 2006;1(6):506-12. doi: http://dx.doi.org/10.1016/S1556-0864(15)30351-8 PMID: 17409909
24. Jassem JR RSantoro A, Schuette W, Chemaissani A, Hong A, Blatter J et al. Phase III Trial of Pemetrexed Plus Best Supportive Care Compared With Best Supportive Care in Previously Treated Patients With Advanced Malignant Pleural Mesothelioma. J Clin Oncol. 2008;26(10):1698-704. doi: http://dx.doi.org/10.1200/JCO.2006.09.9887 PMID: 18375898
Zucali PS M, Michetti G, TiseoM, Ceresoli GL, Collovà E, Follador A, et al. Second-line Chemotherapy in Malignant Pleural Mesothelioma: Results of a Retrospective Multicenter Survey. Lung Cancer. 2011;75(3):360-7. doi: http://dx.doi.org/10.1016/j.lungcan.2011.08.011 PMID: 21937142
Ceresoli GL, Zucali PA, De Vincenzo F, Gianoncelli L, Simonelli M, Lorenzi E, et al. Retreatment with pemetrexed-based chemotherapy in patients with malignant pleural mesothelioma. Lung Cancer. 2011;72(1):73-7. doi: http://dx.doi.org/10.1016/j.lungcan.2010.12.004 PMID: 21216487
Bearz A, Talamini R, Rossoni G, Santo A, de Pangher V, Fasola G, et al. Re-challenge with pemetrexed in advanced mesothelioma: a multi-institutional experience. BMC Res Notes. 2012;5:482. doi: http://dx.doi.org/10.1186/1756-0500-5-482 PMID: 22943698
Zucali PA, Perrino M, Lorenzi E, Ceresoli GL, De Vincenzo F, Simonelli M, et al. Vinorelbine in pemetrexed-pretreated patients with malignant pleural mesothelioma. Lung Cancer. 2014;84(3):265-70. doi: http://dx.doi.org/10.1016/j.lungcan.2013.11.011 PMID: 24321581
Sørensen JB, Langer SW, Urbanska E, Aamdal E. Second-Line Oral Vinorelbine Following First-Line Platinum and Pemetrexed in Malignant Pleural Mesothelioma. Eur J Cancer Clin Oncol. 2012;000(000):1-7. doi: http://dx.doi.org/10.1097/JTO.0b013e31802f3813
Kindler HL, Millard F, Herndon JE, 2nd, Vogelzang NJ, Suzuki Y, Green MR. Gemcitabine for malignant mesothelioma: A phase II trial by the Cancer and Leukemia Group B. Lung Cancer. 2001;31(2-3):311-7. doi: http://dx.doi.org/10.1016/s0169-5002(00)00166-5 PMID: 11165412
Zucali PA, Ceresoli GL, Garassino I, De Vincenzo F, Cavina R, Campagnoli E, et al. Gemcitabine and vinorelbine in pemetrexed-pretreated patients with malignant pleural mesothelioma. Cancer. 2008;112(7):1555-61. doi: http://dx.doi.org/10.1002/cncr.23337 PMID: 18286536
Toyokawa G, Takenoyama M, Hirai F, Toyozawa R, Inamasu E, Kojo M, et al. Gemcitabine and vinorelbine as second-line or beyond treatment in patients with malignant pleural mesothelioma pretreated with platinum plus pemetrexed chemotherapy. Int J Clin Oncol. 2014;19(4):601-6. doi: http://dx.doi.org/10.1007/s10147-013-0619-5 PMID: 24158772
Strizzi L, Catalano A, Vianale G, Orecchia S, Casalini A, Tassi G, et al. Vascular endothelial growth factor is an autocrine growth factor in human malignant mesothelioma. J Pathol. 2001;193(4):468-75. doi: http://dx.doi.org/10.1002/path.824 PMID: 11276005
Masood R, Kundra A, Zhu S, Xia G, Scalia P, Smith DL, et al. Malignant mesothelioma growth inhibition by agents that target the VEGF and VEGF-C autocrine loops. Int J Cancer. 2003;104(5):603-10. doi: http://dx.doi.org/10.1002/ijc.10996 PMID: 12594815
Zalcman G, Margery J, Greillier L, Audigier-Valette C, Moro-Sibilot D, Molinier O, et al. Bevacizumab for newly diagnosed pleural mesothelioma in the Mesothelioma Avastin Cisplatin Pemetrexed Study (MAPS): a randomised, controlled, open-label, phase 3 trial. Lancet. 2016 387(10026):1405-14. doi: http://dx.doi.org/10.1016/S0140-6736(15)01238-6 PMID: 2671923
Ceresoli G, Zucali P, Mencoboni M et al. Phase II study of pemetrexed and carboplatin plus bevacizumab as first-line therapy in malignant pleural mesothelioma. Br J Cancer 2013;109:552-8. doi: http://dx.doi.org/10.1038/bjc.2013.368 PMID: 23860535
Dowell JE, Taub RN, Gerber DE, Ngov L, Yan J, Xie Y, et al. A multicenter phase II study of cisplatin, pemetrexed, and bevacizumab in patients with advanced malignant mesothelioma. Lung Cancer. 2012 77(3):567-71. doi: http://dx.doi.org/10.1016/j.lungcan.2012.05.111 PMID: 2277037
Kindler HL, Karrison TG, Gandara DR, Lu C, Krug LM, Stevenson JP, et al. Multicenter, double-blind, placebo-controlled, randomized phase II trial of gemcitabine/cisplatin plus bevacizumab or placebo in patients with malignant mesothelioma. J Clin Oncol. 2012 Jul 10;30(20):2509-15. doi: http://dx.doi.org/10.1200/JCO.2011.41.5869 PMID: 22665541
Buikhuisen WA, Burgers JA, Vincent AD, Korse CM, van Klaveren RJ, Schramel FM, et al. Thalidomide versus active supportive care for maintenance in patients with malignant mesothelioma after first-line chemotherapy (NVALT 5): an open-label, multicentre, randomised phase 3 study. Lancet Oncol. 2013;14(6):543-51. doi: http://dx.doi.org/10.1016/S1470-2045(13)70125-6 PMID: 23583604
Grosso F, Steele N, Novello S, Nowak AK, Popat S, Greillier L, et al. Nintedanib Plus Pemetrexed/Cisplatin in Patients With Malignant Pleural Mesothelioma: Phase II Results From the Randomized, Placebo-Controlled LUME-Meso Trial. J Clin Oncol. 2017;35(31):3591-600. doi: http://dx.doi.org/10.1200/JCO.2017.72.9012 PMID: 28892431
Scagliotti GV, Gaafar R, Nowak AK, Nakano T, van Meerbeeck J, Popat S, et al. Nintedanib in combination with pemetrexed and cisplatin for chemotherapy-naive patients with advanced malignant pleural mesothelioma (LUME-Meso): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet Respir Med. 2019;7(7):569-80. doi: http://dx.doi.org/10.1016/S2213-2600(19)30139-0. PMID: 31103412
World Health Organization Model List of Essential Medicines, 21st List. Geneva: World Health Organization; 2019. Available from: https://www.who.int/groups/expert-committee-on-selection-and-use-of-essential-medicines/essential-medicines-lists
MacLeod N, Chalmers A, O’Rourke N, Moore K, Sheridan J, McMahon L, et al. Is radiotherapy useful for treating pain in mesothelioma? A phase II trial. J Thorac Oncol. 2015;10(6):944-50. doi: http://dx.doi.org/10.1097/JTO.0000000000000499 PMID: 25654216
Ball DL, Cruickshank DG. Treatment of mesothelioma of the pleura: Review of a 5-Year Experience, With Special Reference to Radiotherapy. Am J Clin Oncol 1990;13(1):4-9. doi: http://dx.doi.org/10.1097/00000421-199002000-00002 PMID: 1689538.
Gomez DR, Rimner A, Simone CB 2nd, Cho BCJ, de Perrot M, Adjei AA, et al. The Use of Radiation Therapy for the Treatment of Malignant Pleural Mesothelioma: Expert Opinion from the National Cancer Institute Thoracic Malignancy Steering Committee, International Association for the Study of Lung Cancer, and Mesothelioma Applied Research Foundation. J Thorac Oncol. 2019;14(7):1172-83. doi: http://dx.doi.org/ 10.1016/j.jtho.2019.03.030 PMID: 31125736
Jenkins P, Milner R, Salmon C. Re-evaluating the role of palliative radiotherapy in malignant pleural mesothelioma. Eur J Cancer. 2011;47(14):2143-9. doi: http://dx.doi.org/10.1016/j.ejca.2011.05.012 PMID: 21658936
de Graaf-Strukowska L, van der Zee J, van Putten W, Senan S.. Factors influencing the outcome of radiotherapy in malignant mesothelioma of the pleura–a single-institution experience with 189 patients. Int J Radiat Oncol Biol Phys. 1999;43(3):511-6. doi: http://dx.doi.org/10.1016/s0360-3016(98)00409-x PMID: 10078630
Bissett D, Macbeth FR, Cram I. The role of palliative radiotherapy in malignant mesothelioma. Clin Oncol 1991;3(6):315-7. doi: http://dx.doi.org/10.1016/s0936-6555(05)80582-5 PMID: 1720658
Price A. What is the role of radiotherapy in malignant pleural mesothelioma? Oncologist. 2011;16(3):359. doi: http://dx.doi.org/10.1634/theoncologist.2010-0185 PMID: 21346022
Chapman E, Diéguez MG. Radiotherapy for malignant pleural mesothelioma. Cochrane Database of Systematic Reviews 2006; (3). doi: http://dx.doi.org/10.1002/14651858.CD003880.pub4 PMID: 16856023
Foroudi F, Smith JG, Putt F, Wada M. High-dose palliative radiotherapy for malignant pleural mesothelioma. J Med Imaging Radiat Oncol. 2017;61(6):797-803. doi: http://dx.doi.org/10.1111/1754-9485.12636 PMID: 28727277
Ashton M, O’Rourke N, Macleod N, Laird B, Stobo J, Kelly C,et al. SYSTEMS-2: A randomised phase II study of radiotherapy dose escalation for pain control in malignant pleural mesothelioma. Clin Trans Radiat Oncol. 2017;8:45-9. doi: http://dx.doi.org/10.1016/j.ctro.2017.11.004 PMID: 29594241
Boutin C, Rey F, Viallat JR. Prevention of malignant seeding after invasive diagnostic procedures in patients with pleural mesothelioma. A randomized trial of local radiotherapy. Chest. 1995;108:754-8. doi: http://dx.doi.org/10.1378/chest.108.3.754 PMID: 7656629
O’Rourke N, Garcia JC, Paul J, Lawless C, McMenemin R, Hill J. A randomised controlled trial of intervention site radiotherapy in malignant pleural mesothelioma. Radiother Oncol. 2007;84:18. doi: http://dx.doi.org/10.1016/j.radonc.2007.05.022 PMID: 17588698
Bydder S, Phillips M, Joseph DJ, Cameron F, Spry NA, DeMelker Y, et al. A randomised trial of single-dose radiotherapy to prevent procedure tract metastasis by malignant mesothelioma. Br J Cancer. 2004;91:9. doi: http://dx.doi.org/10.1038/sj.bjc.6601957 PMID: 15199394
Clive AO, Taylor H, Dobson L, Wilson P, de Winton E, Panakis N, et al. Prophylactic radiotherapy for the prevention of procedure-tract metastases after surgical and large-bore pleural procedures in malignant pleural mesothelioma (SMART): A multicentre, open-label, phase 3, randomised controlled trial. Lancet Oncol. 2016;17:1094-104. doi: http://dx.doi.org/10.1016/S1470-2045(16)30095-X PMID: 27345639
Bayman N, Appel W, Ashcroft L, Baldwin DR, Bates A, Darlison L, et al. Prophylactic Irradiation of Tracts in Patients With Malignant Pleural Mesothelioma: An Open-Label, Multicenter, Phase III Randomized Trial. J Clin Oncol. 2019;37:1200. doi: http://dx.doi.org/10.1200/JCO.18.01678 PMID: 30920878
Rice D, Rusch V, Pass H, Asamura H, Nakano T, Edwards J, et al. Recommendations for uniform definitions of surgical techniques for malignant pleural mesothelioma: a consensus report of the international association for the study of lung cancer international staging committee and the international mesothelioma interest group. J Thorac Oncol. 2011;6(8):1304-12. doi: http://dx.doi.org/10.1097/JTO.0b013e3182208e3f. PMID: 21847060
Yan TD, Tin M, Boyer M, McLean J, G Bannon P, McCaughan BC. Treatment failure after extrapleural pneumonectomy for malignant pleural mesothelioma. J Thorac Dis. 2009 Dec;1(1):23-8 PMID: 22262998
Baldini EH, Richards WG, Gill RR, Goodman BM, Winfrey OK, Eisen HM, et al. Updated patterns of failure after multimodality therapy for malignant pleural mesothelioma. J Thorac Cardiovasc Surg. 2015 May;149(5):1374-81. doi: http://dx.doi.org/10.1016/j.jtcvs.2014.10.128 PMID: 25772281
Cao C, Yan TD, Bannon PG, McCaughan BC. Summary of prognostic factors and patient selection for extrapleural pneumonectomy in the treatment of malignant pleural mesothelioma. Ann Surg Oncol. 2011;18(10):2973-9. doi: http://dx.doi.org/10.1245/s10434-011-1728-x PMID: 21512863
Sugarbaker DJ, Richards WG, Bueno R. Extrapleural pneumonectomy in the treatment of epithelioid malignant pleural mesothelioma: novel prognostic implications of combined N1 and N2 nodal involvement based on experience in 529 patients. Ann Surg. 2014;260(4):577-80; discussion 80-2. doi: http://dx.doi.org/10.1097/SLA.0000000000000903 PMID: 25203873
Nelson DB, Rice DC, Niu J, Atay SM, Vaporciyan AA, Antonoff MB, et al. Predictors of trimodality therapy and trends in therapy for malignant pleural mesothelioma. Eur J Cardiothorac Surg. 2018;53(5):960-6. doi: http://dx.doi.org/10.1093/ejcts/ezx427. PMID: 29211849
Linton A, Pavlakis N, O’Connell R, Soeberg M, Kao S, Clarke S, et al. Factors associated with survival in a large series of patients with malignant pleural mesothelioma in New South Wales. Br J Cancer. 2014;111(9):1860-9. doi: http://dx.doi.org/10.1038/bjc.2014.478. Epub 2014 Sep 4. PMID: 25188323
Treasure T, Lang-Lazdunski L, Waller D, Bliss JM, Tan C, Entwisle J, et al. Extra-pleural pneumonectomy versus no extra-pleural pneumonectomy for patients with malignant pleural mesothelioma: clinical outcomes of the Mesothelioma and Radical Surgery (MARS) randomised feasibility study. Lancet Oncol. 2011;12(8):763-72. doi: http://dx.doi.org/10.1016/S1470-2045(11)70149-8 PMID: 21723781
Cao C, Tian DH, Pataky KA, Yan TD. Systematic review of pleurectomy in the treatment of malignant pleural mesothelioma. Lung Cancer. 2013;81(3):319-27. doi: http://dx.doi.org/10.1016/j.lungcan.2013.04.024. PMID: 23769317
Flores RM, Pass HI, Seshan VE, Dycoco J, Zakowski M, Carbone M, et al. Extrapleural pneumonectomy versus pleurectomy/decortication in the surgical management of malignant pleural mesothelioma: results in 663 patients. J Thorac Cardiovasc Surg. 2008;135(3):620-6, 6 e1-3. doi: http://dx.doi.org/10.1016/j.jtcvs.2007.10.054 PMID: 18329481
Schwartz RM, Lieberman-Cribbin W, Wolf A, Flores RM, Taioli E. Systematic review of quality of life following pleurectomy decortication and extrapleural pneumonectomy for malignant pleural mesothelioma. BMC Cancer. 2018;18(1):1188. doi: http://dx.doi.org/10.1186/s12885-018-5064-4 PMID: 30497433
Rena O, Casadio C. Extrapleural pneumonectomy for early stage malignant pleural mesothelioma: a harmful procedure. Lung Cancer. 2012;77(1):151-5. doi: http://dx.doi.org/10.1016/j.lungcan.2011.12.009 PMID: 22244608
Flores RM, Krug LM, Rosenzweig KE, Venkatraman E, Vincent A, Heelan R, et al. Induction chemotherapy, extrapleural pneumonectomy, and postoperative high-dose radiotherapy for locally advanced malignant pleural mesothelioma: a phase II trial. J Thorac Oncol. 2006 May;1(4):289-95 PMID: 17409872
Lang-Lazdunski L, Bille A, Lal R, Cane P, McLean E, Landau D, et al. Pleurectomy/decortication is superior to extrapleural pneumonectomy in the multimodality management of patients with malignant pleural mesothelioma. J Thorac Oncol. 2012 Apr;7(4):737-43. doi: http://dx.doi.org/10.1097/JTO.0b013e31824ab6c5 PMID: 22425923
Tonoli S, Vitali P, Scotti V, Bertoni F, Spiazzi L, Ghedi B, et al. Adjuvant radiotherapy after extrapleural pneumonectomy for mesothelioma. Prospective analysis of a multi-institutional series. Radiother Oncol. 2011;101:311-5. doi: http://dx.doi.org/10.1016/j.radonc.2011.09.025 PMID: 22079529
De Bondt C, Psallidas I, Van Schil PEY, van Meerbeeck JP. Combined modality treatment in mesothelioma: a systemic literature review with treatment recommendations. Transl Lung Cancer Res. 2018;7(5):562-73. doi: http://dx.doi.org/10.21037/tlcr.2018.10.02 PMID: 30450295
74. Cao C, Tian D, Manganas C.. Systematic review of trimodality therapy for patients with malignant pleural mesothelioma. Ann Cardiothorac Surg. 2012;1(4):428-37. doi: http://dx.doi.org/10.3978/j.issn.2225-319X.2012.11.07 PMID: 23977533
Abdel-Rahman O, Elsayed Z, Mohamed H, Eltobgy M. Radical multimodality therapy for malignant pleural mesothelioma. Cochrane Database Syst Rev. 2018 Jan 8;1(1):CD012605. doi: http://dx.doi.org/10.1002/14651858.CD012605.pub2 PMID: 29309720
NCCN Clinical Practice Guidelines in Oncology: Malignant Pleural Mesothelioma. National Comprehensive Cancer Network; 2020. Available from: https://www.nccn.org/guidelines/category_1
Kindler HL, Ismaila N, Armato SG, 3rd, Bueno R, Hesdorffer M, Jahan T, et al. Treatment of Malignant Pleural Mesothelioma: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2018;36(13):1343-73. doi: http://dx.doi.org/10.1200/JCO.2017.76.6394. Epub 2018 Jan 18. PMID: 29346042
Woolhouse I, Bishop L, Darlison L, De Fonseka D, Edey A, Edwards J, et al. British Thoracic Society Guideline for the investigation and management of malignant pleural mesothelioma. Thorax. 2018;73(Suppl 1):i1-i30. doi: http://dx.doi.org/10.1136/thoraxjnl-2017-211321 PMID: 29444986
Baas P, Fennell D, Kerr KM, Van Schil PE, Haas RL, Peters S, et al. Malignant pleural mesothelioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26 Suppl 5:v31-9. doi: http://dx.doi.org/10.1093/annonc/mdv199 PMID: 26223247
Scherpereel A, Astoul P, Baas P, Berghmans T, Clayson H, de Vuyst P, et al. Guidelines of the European Respiratory Society and the European Society of Thoracic Surgeons for the management of malignant pleural mesothelioma. Eur Respir J. 2010;35(3):479-95. doi: http://dx.doi.org/10.1183/09031936.00063109 PMID: 19717482
81. de Perrot M, Feld R, Cho BC, Bezjak A, Anraku M, Burkes R, , et al. Trimodality therapy with induction chemotherapy followed by extrapleural pneumonectomy and adjuvant high-dose hemithoracic radiation for malignant pleural mesothelioma. J Clin Oncol. 2009;27:1413–8. doi: http://dx.doi.org/10.1200/JCO.2008.17.5604. PMID: 1922485582. Van Schil PE, Baas P, Gaafar R, Maat AP, Van de Pol M, Hasan B, et al. Trimodality therapy for malignant pleural mesothelioma: results from an EORTC phase II multicentre trial. Eur Respir J. 2010;36(6):1362-9. doi: http://dx.doi.org/10.1183/09031936.00039510 PMID: 20525721
Krug LM, Pass HI, Rusch VW, Kindler HL, Sugarbaker DJ, Rosenzweig KE, et al. Multicenter phase II trial of neoadjuvant pemetrexed plus cisplatin followed by extrapleural pneumonectomy and radiation for malignant pleural mesothelioma. J Clin Oncol. 2009;27(18):3007-13. doi: http://dx.doi.org/ 10.1200/JCO.2008.20.3943. PMID: 19364962
Federico R, Adolfo F, Giuseppe M, Lorenzo S, Martino DT, Anna C, et al. Phase II trial of neoadjuvant pemetrexed plus cisplatin followed by surgery and radiation in the treatment of pleural mesothelioma. BMC Cancer. 2013;13:22. doi: http://dx.doi.org/10.1186/1471-2407-13-22. PMID: 23324131
Weder W, Stahel RA, Bernhard J, Bodis S, Vogt P, Ballabeni P, et al. Multicenter trial of neo-adjuvant chemotherapy followed by extrapleural pneumonectomy in malignant pleural mesothelioma. Ann Oncol. 2007;18(7):1196-202. doi: http://dx.doi.org/10.1093/annonc/mdm093 PMID: 17429100
Rusch VW, Rosenzweig K, Venkatraman E, Leon L, Raben A, Harrison L, et al. A phase II trial of surgical resection and adjuvant high-dose hemithoracic radiation for malignant pleural mesothelioma. J Thorac Cardiovasc Surg. 2001;122(4):788-95. doi: http://dx.doi.org/10.1067/mtc.2001.116560 PMID: 11581615
Stahel RA, Riesterer O, Xyrafas A, Opitz I, Beyeler M, Ochsenbein A, et al. Neoadjuvant chemotherapy and extrapleural pneumonectomy of malignant pleural mesothelioma with or without hemithoracic radiotherapy (SAKK 17/04): a randomised, international, multicentre phase 2 trial. Lancet Oncol. 2015;16(16):1651-8. doi: http://dx.doi.org/ 10.1016/S1470-2045(15)00208-9 PMID: 26538423
Allen AM, Czerminska M, Jänne PA, Sugarbaker DJ, Bueno R, Harris JR, , et al. Fatal pneumonitis associated with intensity-modulated radiation therapy for mesothelioma. Int J Radiat Oncol Biol Phys. 2006;65(3):640-5. doi: http://dx.doi.org/10.1016/j.ijrobp.2006.03.012 PMID: 16751058
Rimner A, Zauderer MG, Gomez DR, Adusumilli PS, Parhar PK, Wu AJ, et al. Phase II Study of Hemithoracic Intensity-Modulated Pleural Radiation Therapy (IMPRINT) As Part of Lung-Sparing Multimodality Therapy in Patients With Malignant Pleural Mesothelioma. J Clin Oncol. 2016;34(23):2761-8. doi: http://dx.doi.org/10.1200/JCO.2016.67.2675 PMID: 27325859
Shaikh F, Zauderer, MG, von Reibnitz D, Wu AJ, Yorke ED, Foster A, et al . Improved Outcomes with Modern Lung-Sparing Trimodality Therapy in Patients with Malignant Pleural Mesothelioma. J Thorac Oncol 2017; 12(6):993–1000. doi: http://dx.doi.org/10.1016/j.jtho.2017.02.026 PMID: 28341225
Martin-Ucar AE, Edwards JG, Rengajaran A, Muller S, Waller DA. Palliative surgical debulking in malignant mesothelioma. Predictors of survival and symptom control. Eur J Cardiothorac Surg. 2001;20(6):1117-21. doi: http://dx.doi.org/10.1016/s1010-7940(01)00995-2. PMID: 11717014
Fysh ET, Tan SK, Read CA, Lee F, McKenzie K, Olsen N,et al. Pleurodesis outcome in malignant pleural mesothelioma. Thorax. 2013 Jun;68(6):594-6. doi: http://dx.doi.org/10.1136/thoraxjnl-2012-203043 PMID: 23299964
Dresler CM, Olak J, Herndon JE, 2nd, Richards WG, Scalzetti E, Fleishman SB, et al. Phase III intergroup study of talc poudrage vs talc slurry sclerosis for malignant pleural effusion. Chest. 2005;127(3):909-15. doi: http://dx.doi.org/10.1378/chest.127.3.909 PMID: 15764775
Khoja AM AD, Mulik UP, Seth T. Talc pleurodesis: easy alternative solution. J Bronchology Interv Pulmonol 2004 11(4):226-32. doi: http://dx.doi.org/10.1097/01.lab.0000141898.96929.b3
Thomas R, Francis R, Davies HE, Lee YC.. Interventional therapies for malignant pleural effusions: the present and the future. Respirology. 2014;19(16):809-22. doi: http://dx.doi.org/10.1111/resp.12328 PMID: 24947955
Rintoul RC, Ritchie AJ, Edwards JG, Waller DA, Coonar AS, Bennett M, et al. Efficacy and cost of video-assisted thoracoscopic partial pleurectomy versus talc pleurodesis in patients with malignant pleural mesothelioma (MesoVATS): an open-label, randomised, controlled trial. Lancet. 2014;384(9948):1118-27. doi: http://dx.doi.org/10.1016/S0140-6736(14)60418-9 PMID: 24942631
Azzopardi M, Porcel JM, Koegelenberg CF, Lee YC, Fysh ET. Current controversies in the management of malignant pleural effusions. Semin Respir Crit Care Med. 2014;35(6):723-31. doi: http://dx.doi.org/10.1055/s-0034-1395795 PMID: 25463163
Iyer NP, Reddy CB, Wahidi MM, Lewis SZ, Diekemper RL, Feller-Kopman D, et al. Indwelling Pleural Catheter versus Pleurodesis for Malignant Pleural Effusions. A Systematic Review and Meta-Analysis. Ann Am Thorac Soc. 2019;16(1):124-31. doi: http://dx.doi.org/10.1513/AnnalsATS.201807-495OC PMID: 30272486
Muruganandan S, Azzopardi M, Fitzgerald DB, Shrestha R, Kwan BCH, Lam DCL, et al. Aggressive versus symptom-guided drainage of malignant pleural effusion via indwelling pleural catheters (AMPLE-2): an open-label randomised trial. Lancet Respir Med. 2018;6(9):671-80. doi: http://dx.doi.org/10.1016/S2213-2600(18)30288-1 PMID: 30037711
Van Meter ME, McKee KY, Kohlwes RJ. Efficacy and safety of tunneled pleural catheters in adults with malignant pleural effusions: a systematic review. J Gen Intern Med. 2011;26(1):70-6. doi: http://dx.doi.org/ 10.1007/s11606-010-1472-0 PMID: 20697963
Mekhaiel E, Kashyap R, Mullon JJ, Maldonado F. Infections associated with tunnelled indwelling pleural catheters in patients undergoing chemotherapy. J Bronchology Interv Pulmonol. 2013;20(4):299-303. doi: http://dx.doi.org/10.1097/LBR.0000000000000001 PMID: 24162111102
Morel A, Mishra E, Medley L, Rahman NM, Wrightson J, Talbot D, et al. Chemotherapy should not be withheld from patients with an indwelling pleural catheter for malignant pleural effusion. Thorax. 2011;66(5):448-9. doi: http://dx.doi.org/10.1136/thx.2009.133504 PMID: 20880866
Lui MM, Thomas R, Lee YC. Complications of indwelling pleural catheter use and their management. BMJ Open Respir Res. 2016;3(1):e000123. doi: http://dx.doi.org/10.1136/bmjresp-2015-000123 PMID: 26870384
World Health Organisation. WHO Definition of Palliative Care Geneva: WHOAvailable from: https://www.who.int/cancer/palliative/definition/en/.
Knaul FF P, Krakauer E, De Lima L, Bhadelia A Kwete X, Arreola-Ornelas H, et la.. Alleviating the access abyss in palliative care and pain relief-an imperative of universal health coverage: The Lancet Commission report. Lancet. 2007;391:1391–454. doi: http://dx.doi.org/10.1016/S0140-6736(17)32513-8 PMID: 29032993
Merskey H. Classification of Chronic Pain. 2nd ed. Seattle: IASP Press; 1994. Available from: https://www.iasp-pain.org/PublicationsNews/Content.aspx?ItemNumber=1673
Saunders JA M, Hall C, Laird B, MacLeod N. Pain management in patients with malignant mesothelioma: challenges and solutions. Lung Cancer: Targets and Therapy. 2019;10:37-46. doi: http://dx.doi.org/10.2147/LCTT.S192558 PMID: 31037036
Ventafridda V, Saita L, Ripamonti C, De Conno F. WHO guidelines for the use of analgesics in cancer pain. Int J Tissue React. 1985;7(1):93-6. PMID: 2409039
Salminen EK, Silvoniemi M, Syrjänen K, Kaasa S, Kloke M, Klepstad P. Opioids in pain management of mesothelioma and lung cancer patients. Acta Oncol. 2013 Jan;52(1):30-7. doi: http:/dx.doi.org/10.3109/0284186X.2012.725944 PMID: 23025295
Wong FC, Lee TW, Yuen KK, Lo SH, Sze WK, Tung SY. Intercostal nerve blockade for cancer pain: effectiveness and selection of patients. Hong Kong Med J. 2007 Aug;13(4):266-70 PMID: 17664531
France BD, Lewis RA, Sharma ML, Poolman M. Cordotomy in mesothelioma-related pain: a systematic review. BMJ Support Palliat Care. 2014 Mar;4(1):19-29. doi: http://dx.doi.org/10.1136/bmjspcare-2013-000508 PMID: 24644767
Luckett T, Phillips J, Johnson MJ, Farquhar M, Swan F, Assen T,et al. Contributions of a hand-held fan to self-management of chronic breathlessness. Eur Respir J 2017;50 1700262. doi: http://dx.doi.org/10.1183/13993003.00262-2017 PMID: 28818884
Galbraith S, Fagan P, Perkins P, Lynch A, Booth S. Does the use of a handheld fan improve chronic dyspnea? A randomized,controlled, crossover trial. J Pain Symptom Mgt 2010;39:831-8. doi: http://dx.doi.org/ 10.1016/j.jpainsymman.2009.09.024 PMID: 20471544114.
Baltzan MA AA, Rotaple M, et al. Fan to palliate exercise-induced dyspnoea with severe COPD. Am J Resp Crit Care Med. 2000;161(3 Suppl):A59.
Gamborg H, Riis J, Christrup L, Krantz T. Effect of intraoral and subcutaneous morphine on dyspnea at rest in terminal patients with primary lung cancer or lung metastases. J Opioid Manag. 2013 Jul-Aug;9(4):269-74. doi: http://dx.doi.org/ 10.5055/jom.2013.0168 PMID: 24353020
Abernethy AP, McDonald CF, Frith PA, Clark K, Herndon JE 2nd, Marcello J, et al. Effect of palliative oxygen versus room air in relief of breathlessness in patients with refractory dyspnoea: a double-blind, randomised controlled trial. Lancet. 2010 Sep 4;376(9743):784-93. doi: http://dx.doi.org/10.1016/S0140-6736(10)61115-4 PMID: 20816546
Jennings AL, Davies AN, Higgins JP, Gibbs JS, Broadley KE. A systematic review of the use of opioids in the management of dyspnoea. Thorax. 2002 Nov;57(11):939-44. doi: http://dx.doi.org/10.1136/thorax.57.11.939. PMID: 12403875
Simon ST, Higginson IJ, Booth S, Harding R, Weingärtner V, Bausewein C. Benzodiazepines for the relief of breathlessness in advanced malignant and non-malignant diseases in adults. Cochrane Database Syst Rev. 2016 Oct 20;10(10):CD007354. doi: http://dx.doi.org/10.1002/14651858.CD007354.pub3 PMID: 27764523
Molassiotis A, Bailey C, Caress A, Tan JY. Interventions for cough in cancer. Cochrane Database Syst Rev. 2015 May 19;5(5):CD007881. doi: http://dx.doi.org/ 10.1002/14651858.CD007881.pub3 PMID: 25989380120.
Forde PM, Sun Z, Anagnostou V, Kindler HL, Purcell WT, Goulart BH, et al. PrE0505: Phase II multicenter study of anti-PD-L1, durvalumab, in combination with cisplatin and pemetrexed for the first-line treatment of unresectable malignant pleural mesothelioma (MPM)—A PrECOG LLC study. [ASCO abstract 9003]. J Clin Oncol.38(15 (suppl) doi: http://dx.doi.org/10.1200/JCO.2020.38.15_suppl.9003
Nowak AK, Lesterhuis WJ, Kok PS, Brown C, Hughes BG, Karikios DJ, et al. Durvalumab with first-line chemotherapy in previously untreated malignant pleural mesothelioma (DREAM): a multicentre, single-arm, phase 2 trial with a safety run-in. Lancet Oncol. 2020 Sep;21(9):1213-1223. doi: http://dx.doi.org/10.1016/S1470-2045(20)30462-9 PMID: 32888453
Desai A KT, Rose B, Tan Y, Hill B, Pemberton E, Straus C,et al. OA08. 03 phase II trial of pembrolizumab (NCT02399371) in previously-treated malignant mesothelioma (MM): final analysis. J Thorac Oncol. 2018;13(10):S339. doi: http://doi.org/10.1016/j.jtho.2018.08.277
Metaxas Y, Rivalland G, Mauti LA, Klingbiel D, Kao S, Schmid S, et al. Pembrolizumab as Palliative Immunotherapy in Malignant Pleural Mesothelioma. J Thorac Oncol. 2018 Nov;13(11):1784-1791. doi: http://dx.doi.org/ 10.1016/j.jtho.2018.08.007 PMID: 30142389
Okada M, Kijima T, Aoe K, Kato T, Fujimoto N, Nakagawa K, et al. Clinical Efficacy and Safety of Nivolumab: Results of a Multicenter, Open-label, Single-arm, Japanese Phase II study in Malignant Pleural Mesothelioma (MERIT). Clin Cancer Res. 2019 Sep 15;25(18):5485-5492. doi: http://dx.doi.org/10.1158/1078-0432.CCR-19-0103 PMID: 31164373
Quispel-Janssen J, van der Noort V, de Vries JF, Zimmerman M, Lalezari F, Thunnissen E, Monkhorst K, et al. Programmed Death 1 Blockade with Nivolumab in Patients With Recurrent Malignant Pleural Mesothelioma. J Thorac Oncol. 2018 Oct;13(10):1569-1576. doi: http://dx.doi.org/10.1016/j.jtho.2018.05.038 PMID: 29908324
Maio M, Scherpereel A, Calabrò L, Aerts J, Perez SC, Bearz A, et al. Tremelimumab as second-line or third-line treatment in relapsed malignant mesothelioma (DETERMINE): a multicentre, international, randomised, double-blind, placebo-controlled phase 2b trial. Lancet Oncol. 2017 Sep;18(9):1261-1273. doi: http://dx.doi.org/10.1016/S1470-2045(17)30446-1 PMID: 28729154
Scherpereel A, Mazieres J, Greillier L, Lantuejoul S, Dô P, Bylicki O, et al. French Cooperative Thoracic Intergroup. Nivolumab or nivolumab plus ipilimumab in patients with relapsed malignant pleural mesothelioma (IFCT-1501 MAPS2): a multicentre, open-label, randomised, non-comparative, phase 2 trial. Lancet Oncol. 2019 Feb;20(2):239-253. doi: http://dx.doi.org/10.1016/S1470-2045(18)30765-4 PMID: 30660609
Popat S, Curioni-Fontecedro A, Dafni U, Shah R, O’Brien M, Pope A, et al. A multicentre randomised phase III trial comparing pembrolizumab versus single-agent chemotherapy for advanced pre-treated malignant pleural mesothelioma: the European Thoracic Oncology Platform (ETOP 9-15) PROMISE-meso trial. Ann Oncol. 2020 Dec;31(12):1734-1745. doi: http://dx.doi.org/10.1016/j.annonc.2020.09.009 PMID: 32976938
Baas P, Scherpereel A, Nowak AK, Fujimoto N, Peters S, Tsao AS, et al. et al. ID: 2908 First-Line Nivolumab+ Ipilimumab vs Chemotherapy in Unresectable Malignant Pleural Mesothelioma: CheckMate 743. J Thorac Oncol. 2020;15(10):e42. doi: http://dx.doi.org/ 10.1016/S0140-6736(20)32714-8 PMID: 33485464
Hassan R, Thomas A, Nemunaitis JJ, Patel MR, Bennouna J, Chen FL, et al. Efficacy and Safety of Avelumab Treatment in Patients with Advanced Unresectable Mesothelioma: Phase 1b Results From the JAVELIN Solid Tumor Trial. JAMA Oncol. 2019 Mar 1;5(3):351-357. doi: http://dx.doi.org/10.1001/jamaoncol.2018.5428 PMID: 30605211
Alley EW, Lopez J, Santoro A, Morosky A, Saraf S, Piperdi B, van Brummelen E. Clinical safety and activity of pembrolizumab in patients with malignant pleural mesothelioma (KEYNOTE-028): preliminary results from a non-randomised, open-label, phase 1b trial. Lancet Oncol. 2017 May;18(5):623-630. doi: htpp://dx.doi.org/10.1016/S1470-2045(17)30169-9. PMID: 28291584
Fennell D, Ottensmeier C, Califano R, Hanna G, Ewings S, Hill K, et al. PS01. 11 Nivolumab Versus Placebo in Relapsed Malignant Mesothelioma: The CONFIRM Phase 3 Trial. Journal of Thoracic Oncology. 2021 Mar 1;16(3):S62 doi: http://dx.doi.org/10.1016/j.jtho.2021.01.323
Calabrò L, Morra A, Giannarelli D, Amato G, D’Incecco A, Covre A, et al. Tremelimumab combined with durvalumab in patients with mesothelioma (NIBIT-MESO-1): an open-label, non-randomised, phase 2 study. Lancet Respir Med. 2018 Jun;6(6):451-460. doi: http://dx.doi.org/10.1016/S2213-2600(18)30151-6 PMID: 29773326
Disselhorst MJ, Quispel-Janssen J, Lalezari F, Monkhorst K, de Vries JF, van der Noort V, et al. Ipilimumab and nivolumab in the treatment of recurrent malignant pleural mesothelioma (INITIATE): results of a prospective, single-arm, phase 2 trial. Lancet Respir Med 2019 7(3):260-70. doi: http://dx.doi.org/10.1016/S2213-2600(18)30420-X
Kindler HL, Ismaila N, Armato SG 3rd, Bueno R, Hesdorffer M, Jahan T, et al. Treatment of Malignant Pleural Mesothelioma: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2018 May 1;36(13):1343-1373. doi: http://dx.doi.org/10.1200/JCO.2017.76.6394 PMID: 29346042136.
Zeltsman M, Dozier J, McGee E, Ngai D, Adusumilli PS. CAR T-cell therapy for lung cancer and malignant pleural mesothelioma. Transl Res. 2017 Sep;187:1-10. doi: http://dx.doi.org/10.1016/j.trsl.2017.04.004 PMID: 28502785
Belderbos RA, Vroman H, Aerts JG. . Cellular Immunotherapy and Locoregional Administration of CAR T-Cells in Malignant Pleural Mesothelioma. Front Oncol. 2020;10 (777):1-11 doi: http://dx.doi.org/10.3389/fonc.2020.00777 PMID: 32582537
Mun EJ, Babiker HM, Weinberg U, Kirson ED, Von Hoff DD. Tumor-Treating Fields: A Fourth Modality in Cancer Treatment. Clin Cancer Res. 2018 Jan 15;24(2):266-275. doi: http://dx.doi.org/10.1158/1078-0432.CCR-17-1117 PMID: 28765323
Stupp R, Taillibert S, Kanner A, Read W, Steinberg D, Lhermitte B, et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma: A Randomized Clinical Trial. JAMA. 2017 Dec 19;318(23):2306-2316. doi: Http://dx.doi.org/10.1001/jama.2017.18718 PMID: 29260225
Kirson ED, Dbalý V, Tovarys F, Vymazal J, Soustiel JF, Itzhaki A, et al. Alternating electric fields arrest cell proliferation in animal tumor models and human brain tumors. Proc Natl Acad Sci U S A. 2007 Jun 12;104(24):10152-7. doi: http://dx.doi.org/10.1073/pnas.0702916104 PMID: 17551011
Chang E, Patel CB, Pohling C, Young C, Song J, Flores TA, et al. Tumor treating fields increases membrane permeability in glioblastoma cells. Cell Death Dis 2018;4(1):1-3. doi: http://dx.doi.org/10.1158/1538-7445.AM2019-250
Ceresoli GL, Aerts JG, Dziadziuszko R, Ramlau R, Cedres S, van Meerbeeck JP, et al. Tumour Treating Fields in combination with pemetrexed and cisplatin or carboplatin as first-line treatment for unresectable malignant pleural mesothelioma (STELLAR): a multicentre, single-arm phase 2 trial. Lancet Oncol. 2019 Dec;20(12):1702-1709. doi: http://dxd.oi.org/10.1016/S1470-2045(19)30532-7 PMID: 31628016
Kolls J, Freeman S, Ramesh R, et al. The treatment of malignant pleural mesothelioma with gene modified cancer cells: a phase I study. Am J Respir Crit Care Med 1998;157:A563?
Molnar-Kimber KL, Sterman DH, Chang M, et al. Humoral and cellular immune responses induced by adenoviral-based gene therapy for localized malignancy: results of a phase 1 clinical trial for malignant mesothelioma. Hum Gene Ther 1998;9:2121–2133. doi: http://dx.doi.org/10.1089/hum.1998.9.14-2121
Sterman DH, Treat J, Litzky LA, et al. Adenovirus-mediated herpes simplex virus thymidine kinase gene delivery in patients with localized malignancy: results of a phase 1 clinical trial in malignant mesothelioma. Hum Gene Ther 1998;9:1083–1092. doi: http://dx.doi.org/10.1089/hum.1998.9.7-1083. PMID: 9607419.
Sterman DH, Recio A, Molnar-Kimber K, et al. Herpes simplex virus thymidine kinase (HSVtk) gene therapy utilizing an E1/E4-deleted adenoviral vector: preliminary results of a phase I clinical trial for pleural mesothelioma. Am J Respir Crit Care Med 1999;159:A237
Sterman DH, Recio A, Vachani A, Sun J, Cheung L, DeLong P, et al. Long-term follow-up of patients with malignant pleural mesothelioma receiving high-dose adenovirus herpes simplex thymidine kinase/ganciclovir suicide gene therapy. Clin Cancer Res 2005; 11: 7444-53 doi: http://dx.doi.org/10.1158/1078-0432.CCR-05-0405 PMID: 16243818.
Sterman DH, Recio A, Carroll RG, Gillespie CT, Haas A, Vachani A, et al. A phase I clinical trial of single-dose intrapleural IFN-β gene transfer for malignant pleural mesothelioma and metastatic pleural effusions. high rate of antitumor immune responses. Clin Cancer Res 2007; 13: 4456–4466. 7453. doi: http://dx.doi.org 10.1158/1078-0432.CCR-07-0403 PMID: 17671130.
Sterman DH, Haas A, Moon E, Recio A, Schwed D, Vachani A, et al. A trial of intrapleural adenoviral-mediated interferon-α2b gene transfer for malignant pleural mesothelioma. Am J Respir Crit Care Med 2011; 184: 1395–1399. doi: http://dx.doi.org/ 10.1164/rccm.201103-0554CR PMID: 21642245
Tagawa M, Tada Y, Shimada H, et al. Gene therapy for malignant mesothelioma: Current prospects and challenges. Cancer Gene Ther 2013; 20, 150–156.. doi: http://dx.doi.org/ 10.1038/cgt.2013.1 PMID: 23392201.
Friedberg JS, Mick R, Stevenson J, Metz J, Zhu T, Buyske J, et al. A phase I study of Foscan-mediated photodynamic therapy and surgery in patients with mesothelioma. Ann Thorac Surg . 2003 Mar 1;75(3):952-9 doi: http://dx.doi.org/10.1016/s0003-4975(02)04474-0 PMID: 1264572
Friedberg JS, Culligan MJ, Mick R, Stevenson J, Hahn SM, Sterman D, et al.. Radical pleurectomy and intraoperative photodynamic therapy for malignant pleural mesothelioma. Ann Thorac Surg . 2012 May 1;93(5):1658-67. doi: http://dx.doi.org/ 10.1016/j.athoracsur.2012.02.009 PMID: 22541196
Friedberg JS, Simone II CB, Culligan MJ, Barsky AR, Doucette A, McNulty S, et al. Extended pleurectomy-decortication–based treatment for advanced stage epithelial mesothelioma yielding a median survival of nearly three years. Ann Thorac Surg. 2017 Mar 1;103(3):912-9. doi: http://dx.doi.org/10.1016/j.athoracsur.2016.08.071 PMID: 27825687
Matzi V, Maier A, Sankin O, et al. Photodynamic therapy enhanced by hyperbaric oxygenation in palliation of malignant pleural mesothelioma: clinical experience. Photodiagnosis Photodyn Ther. 2004;1(1):57-64 doi: http://dx.doi.org/ 10.1016/S1572-1000(04)00009-2 PMID: 25048065
Moskal TL, Dougherty TJ, Urschel JD, Antkowiak JG, Regal AM, Driscoll DL, et al. Operation and photodynamic therapy for pleural mesothelioma: 6-year follow-up. Ann Thorac Surg. 1998 Oct 1;66(4):1128-33. doi: http://dx.doi.org/10.1016/s0003-4975(98)00799-1 PMID: 980079
Munck C, Mordon SR, Scherpereel A, Porte H, Dhalluin X, Betrouni N. Intrapleural photodynamic therapy for mesothelioma: what place and which future?Ann Thorac Surg 2015 Jun 1;99(6):2237-45. doi: http://dx.doi.org/ 10.1016/j.athoracsur.2014.12.077 PMID: 25912746
Pass HI, Temeck BK, Kranda K, et al.Phase III randomized trial of surgery with or without intraoperative photodynamic therapy and postoperative immunochemotherapy for malignant pleural mesothelioma. Ann Surg Oncol 1997, 4:628–633 doi: http://dx.doi.org/10.1007/BF02303746 PMID: 9416409
Schouwink H, Rutgers ET, van der Sijp J, Oppelaar H, van Zandwijk N, van Veen R, et al. Intraoperative photodynamic therapy after pleuropneumonectomy in patients with malignant pleural mesothelioma: dose finding and toxicity results. Chest. 2001 Oct 1;120(4):1167-74. doi: http://dx.doi.org/10.1378/chest.120.4.1167 PMID: 11591556
Adusumilli PS, Zauderer MG, Rusch VW, O’Cearbhaill RE, Zhu A, Ngai DA, et al. Abstract CT036: A phase I clinical trial of malignant pleural disease treated with regionally delivered autologous mesothelin-targeted CAR T cells: Safety and efficacy. doi: http://dx.doi.org/ 10.1158/1538-7445.AM2019-CT036
Beatty GL, Haas AR, Maus MV, Torigian DA, Soulen MC, Plesa G, et al. Mesothelin-specific chimeric antigen receptor mRNA-engineered T cells induce antitumor activity in solid malignancies. Cancer Immunol Res . 2014 Feb 1;2(2):112-20. doi: http://dx.doi.org/10.1158/2326-6066.CIR-13-0170 PMID: 24579088
Belderbos RAVH, Aerts JG.Cellular Immunotherapy and Locoregional Administration of CAR T-Cells in Malignant Pleural Mesothelioma. Front Oncol. 2020;10 (777):1-11 doi: http://dx.doi.org/ 10.3389/fonc.2020.00777 PMID: 32582537
Curioni A, Britschgi C, Hiltbrunner S, Bankel L, Gulati P, Weder W, et al. 1226P A phase I clinical trial of malignant pleural mesothelioma treated with locally delivered autologous anti-FAP-targeted CAR T-cells. Ann Oncol. 2019 Oct 1;30(Supplement_5):mdz253-052. doi: http://dx.doi.org/10.1093/annonc/mdz253.052
Haas AR, Tanyi JL, O’Hara MH, Gladney WL, Lacey SF, Torigian DA, et al. Phase I study of lentiviral-transduced chimeric antigen receptor-modified T cells recognizing mesothelin in advanced solid cancers. Mol Ther . 2019 Nov 6;27(11):1919-29. doi: http://dx.doi.org/10.1016/j.ymthe.2019.07.015
Zeltsman M, Dozier J, McGee E, Ngai D, Adusumilli PS. CAR T-cell therapy for lung cancer and malignant pleural mesothelioma. Transl Res. 2017 Sep 1;187:1-0. doi: http://dx.doi.org/10.1016/j.trsl.2017.04.004 PMID: 28502785
Ceresoli GL, Aerts JG, Dziadziuszko R, Ramlau R, Cedres S, van Meerbeeck JP,et al. Tumour Treating Fields in combination with pemetrexed and cisplatin or as first-line treatment for unresectable malignant pleural mesothelioma (STELLAR): a multicentre, single-arm phase 2 trial. Lancet Oncol. 2019 Dec 1;20(12):1702-9. doi: http://dx.doi.org/10.1016/S1470-2045(19)30532-7 PMID: 31628016
Chang E, Patel CB, Pohling C, Young C, Song J, Flores TA, et al. Tumor treating fields increases membrane permeability in glioblastoma cells. Cell Death Discov. 2018 Dec 5;4(1):1-3. doi: http://dx.doi.org/10.1038/s41420-018-0130-x
Kirson ED, Dbalý V, Tovaryš F, Vymazal J, Soustiel JF, Itzhaki A, et al. Alternating electric fields arrest cell proliferation in animal tumor models and human brain tumors. Proc Natl Acad Sci. 2007 Jun 12;104(24):10152-7. doi: http://dx.doi.org/10.1073/pnas.0702916104 PMID: 17551011
Stupp R, Taillibert S, Kanner A, Read W, Steinberg DM, Lhermitte B, et al. Effect of tumor-treating fields plus maintenance temozolomide vs maintenance temozolomide alone on survival in patients with glioblastoma: a randomized clinical trial. JAMA. 2017 Dec 19;318(23):2306-16. doi: http://dx.doi.org/10.1001/jama.2017.18718 PMID: 29260225