ADDRI is an independent, not-for-profit research institute committed to reducing and ultimately eliminating the impact of asbestos and dust-related diseases worldwide.
Our team of doctors, researchers, scientists, nurses and industry leaders excel in innovative thinking and strive for excellence every day.
The importance of collaboration
We are on a mission to collaborate with those working toward the elimination of asbestos and dust-related diseases.
About the Diseases
Asbestos and dust diseases remain a clear and present danger. 4,000 Australians die each year from asbestos-related diseases. It is estimated that one in four workers are at risk of silica-related disease.
Asbestos is a type of mineral made up of tiny, needle-like fibers. Known for its ability to resist heat, electricity, and corrosion, it was widely used in many construction materials. Inhalation of asbestos fibres can directly lead to disease and a form of cancer called mesothelioma.
What is Silica?
Crystalline silica is a natural mineral found in sand, stone, concrete and mortar. Found in high quantities in materials commonly used for tunnel construction and engineered stone, inhalation of silica dust particles can cause serious disease.
Research
We are on a mission to understand asbestos and dust-related disease development and diagnosis through dedicated research. Our evidence-led research drives advancements in medical and scientific understanding and guides our global education and training initiatives.
We are unrelenting in exploring every avenue that will achieve our mission of improving patient outcomes, uncovering new treatments and ultimately ending all asbestos and dust-related diseases.
Working globally
Our status as the WHO Collaborating Centre for Elimination of Asbestos-Related Diseases ensures that our dedication, research and collaboration will have significant impact around the world.
Support
We are on a mission to support people impacted by dust-related diseases. Our Mesothelioma and Silicosis Support Service addresses the needs of patients suffering dust-related diseases and supports their families.
Our specialist nurses are here to address the needs of our patients with mesothelioma and to support carers and families. We can answer any questions you may have and help you navigate the health system
Silicosis support
Emotional and practical support for individuals diagnosed with silicosis and their caregivers.
Education
We are on a mission to educate that asbestos is a very real threat to people all over the world and provide the knowledge and tools to care for those impacted.
An internationally recognised eToolkit on asbestos-related diseases (ARDs), important research to fill knowledge gaps on the elimination of asbestos and much needed training on ARDs in developing countries.
Mesothelioma learning module
Access online training for nurses/health care professionals to assist with diagnosing and caring for patients with mesothelioma.
This section is targeted at nurses, allied health professionals and health practitioners of any field wishing to advance their knowledge of supporting and caring for patients with asbestos-related diseases (ARD) and in particular malignant pleural mesothelioma (MPM). MPM is the deadliest of all ARD’s. The language used in this Chapter is intentionally simple and descriptive, to enable ease of understanding, as is The Cancer Council of Australia’s booklet, Understanding Mesothelioma (1). Any reference to ‘patient(s)’ automatically includes the carer and family members of that patient.
The management of presenting symptoms of MPM in any country varies according to clinician knowledge, clinician skills and access to quality technological services such as radiological imaging and diagnostic essentials (microscopes and immunohistochemical staining). However, without a level of awareness that someone may have been exposed to asbestos and therefore may be displaying symptoms of an asbestos-related disease, a diagnosis of MPM will be missed.
There is a need to exclude common causes of respiratory symptoms such as infections like pneumonia and tuberculosis, other benign respiratory illnesses, as well as viral influenza and COVID-19. There is also the need to exclude other malignancies, such as primary lung cancer and metastatic disease from other cancers like breast, bowel, gastrointestinal tract, and unknown causes.
Mesothelioma is a complex disease. It is preventable, it is incurable, it is difficult to diagnose and there are limited treatment options. Overall survival has remained unchanged over many years and is reported to be around 8-12 months (2, 3). In countries that are resource limited, people are more likely to present with multiple symptoms related to advanced disease that has been undiagnosed for long periods and/or have symptoms of an aggressive and rapidly growing tumour. This can be indicative of the cell type of the mesothelioma. Some people may have slow tumour activity and live with disease without symptoms for longer periods, sometimes years with or without treatment. The priority of care for people with mesothelioma is to minimize symptoms of the disease, treatment, and maximise quality of living. It is important to encourage people to live with normality in their life for as long as possible, seek help when emotions like sadness, hopelessness, depression arise but also acknowledge the need to prepare for a dignified end of life.
In developing countries, where health professional, government, and public knowledge and experience of mesothelioma is limited, the options for management are likely to be minimal, therefore the focus must always be on patient safety, symptom relief and best available care.
Multidisciplinary teams
In Australia likely representing a more favourable than most developing countries, a cancer patient will have access to specialty clinicians working within a specialist multidisciplinary team or MDT. MDTs are usually disease specific, but mesothelioma commonly fits in to a Lung Cancer MDT.
Key members of a Lung Cancer MDT include:
Experienced radiologists providing high grade imaging that includes X-Ray, CT Scanning and PET scanning where some are highly trained interventional radiologists.
Respiratory consultants performing initial assessments, referrals and some are trained in interventional techniques.
Complementing respiratory and radiology are experienced pathologists providing complex cytology, histopathology and immunohistochemistry services leading to an initial diagnosis and then where appropriate ongoing molecular information to inform treatment planning and management.
Cardiothoracic surgeons experienced in video assisted surgery and open radical surgery are valuable MDT members but are not always accessible in all areas.
Experienced medical and radiation oncologists are pivotal to the MDT to provide evidence-based knowledge and treatment.
The patient and family must be supported by an integrative and supportive services that combines palliative care with integrative and complimentary services to minimise symptoms of the disease and treatment and ultimately ensures the patient and their family are prepared as well as possible for an early death.
Integral members of the MDT are inpatient and outpatient nurses in oncology and surgery, along with expert care provided by allied health professionals such as the dietitian, occupational therapist, clinical psychologist, social worker, and exercise physiologist. These members all contribute to the overall wellbeing of the patient by assisting patients to prepare for treatment and manage side effects, whilst aiming to maintain optimal nutrition, physical functionality, personal safety and understand fluctuations in their emotional state.
Access to telehealth technologies for communication and consultations between patients and their treating consultants, nurses and allied health members is beneficial when patients are receiving treatment and care from experienced centres far from home. The aim of all MDT members is to reduce the symptom burden of the disease to enable the patient to live as well as, and as long as possible, with the disease and through treatment.
A lung cancer multidisciplinary team (MDT) should consist of:
Respiratory Specialists: General, interventional, and EBUS (endobronchial ultrasound)
Radiologists: CT Imaging, PET imaging, Interventional care (for drainage and tissue biopsy)
Anatomical Pathologist
Medical Oncologist
Radiation Oncologist
Cardiothoracic Surgeon
Supportive and Integrative Care / Palliative Care Specialist
Specialist Nurse
Reporting to: Local General Practitioner
Referral access to: Dietitian, Exercise Physiologist, Occupational Therapist, and Clinical Psychologist or Social Worker
Symptoms that lead to a diagnosis of MPM
The common presenting symptoms of people with MPM are:
Shortness of breath
Thoracic pain
Weight loss, decreased appetite
Fatigue
Night sweats
1. Shortness of breath
The most common presenting symptom that drives the patient to seek medical assistance is shortness of breath (SOB), often associated with a pleural effusion. A pleural effusion is an abnormal volume of fluid collecting in the pleural space, the space between the two membranes that line the lung (visceral) and chest wall (parietal). The build-up of fluid in the pleural cavity results in a slowly progressive feeling of not being able to get ones breathe especially during exertion or exercise.
For example, a person might report having to take more frequent rests during shopping in their local markets and completing outside activities, but SOB can be characterised by a rapid onset. The patient often follows a health pathway that may span some months of consultations, investigations, and action before a diagnosis of mesothelioma is made.
SOB in the asbestos setting can be associated with asbestosis. Asbestosis is a benign (non-cancer) process that causes progressive and irreversible damage where the irritation of the asbestos fibres cause scarring within the lung tissue.
It is important to reiterate that if there is no community or professional awareness about the dangers of asbestos and exposure to asbestos then the ability to diagnose an ARD will be missed. This is not just a problem for developing countries. It is also an issue in developed countries like Australia, New Zealand, USA, and UK who regularly diagnose and treat mesothelioma. There needs to be a heightened level of awareness about the potential for an ARD diagnosis to be considered.
How is mesothelioma diagnosed?
At the initial presentation to a health practitioner the patient will undergo a clinical examination and will often be prescribed an antibiotic because the presumed cause of SOB is chest infection. It is not uncommon for the patient to re-present to the practitioner with no improvement in SOB or even worsening symptoms despite the antibiotics. At this point the doctor is likely to request imaging, beginning with a chest X-ray. Depending on how the local health care systems work, the patient may find themselves in a hospital emergency department or better still a respiratory service with a chest X-ray demonstrating a pleural effusion.
How is the initial pleural effusion managed?
Management of a pleural effusion is dependent on available medical knowledge and skills, patient location and services availability at that location.
The priority of care is to drain the fluid as an initial procedure and have the fluid analysed for cell culture and cytology. Drainage should be performed by an experienced respiratory physician, an experienced interventional radiologist, or an experienced emergency doctor who is accredited to perform the procedure (thoracentesis or pleural tap) with safety and according to protocol.
After drainage, a repeat chest X-ray is required to assess the adequacy of the aspiration, the degree of lung re-expansion and check for absence of pneumothorax. Patients usually report a significant improvement in their ability to get their breathe after the initial drainage.
Cytology analysis alone is less likely to provide a diagnosis of mesothelioma than a tissue biopsy, so malignancy can never be excluded at this time. It is common for fluid to recur necessitating further action (4).
Further reading:
Guidelines for the Diagnosis and Treatment of Malignant Pleural Mesothelioma (5)
Management of recurrent symptoms and fluid
Management depends on the patient’s circumstances, available health care personnel and resources, such as who can do a procedure? Where the patient is? and what services are available. However, further drainage should be arranged, more fluid sent for culture and cytology, a high-resolution CT scan should be performed, and the patient referred to a specialist service to consult with either a respiratory physician and or interventional radiologist or cardiothoracic surgeon. Management should focus on controlling the fluid by preventing further accumulation, obtaining a diagnosis thereby understanding the cause for the fluid, and maximising respiratory function by performing whatever procedure achieves the best outcome for the patient.
An important consideration in determining management should be around how long the patient can reliably be expected to live. For example, an active middle-aged person deemed to have early disease should be offered definitive fluid control, ideally by surgery, so they can return to quality independent living with appropriate ongoing follow up and where feasible can return to work. Others may have less invasive procedures nevertheless with the ultimate aim of managing the fluid.
Options for managing ongoing fluid recurrence
The following options will vary according to services and skills available.
Interventional Radiologist: Under intravenous sedation and local anaesthetic, a CT guided drainage of fluid and tissue biopsy is performed.
Respiratory Physician: via interventional means using intravenous sedation and local anaesthetic a pleuroscopy is performed. A chest drain is inserted, and the recurrent fluid is drained. If appropriate a biopsy is taken. Pleural fluid is sent for culture and cytology. If able, a talc slurry is introduced to promote a pleurodesis. There is a higher chance of obtaining a diagnosis with a tissue biopsy than by cytology alone (4).
Cardiothoracic Surgeon: Surgery provides an opportunity to drain the fluid, obtain an optimal tissue biopsy, perform talc pleurodesis, maximise lung re-expansion following the procedure and visualise the disease within the chest cavity. It is performed under a general anaesthetic by either video assisted thoracoscopy (VAT) or open thoracotomy:
VAT a standard biopsy is taken, visible tumour is debulked via pleurectomy and decortication and talc is instilled to promote a pleurodesis. The chance of obtaining a diagnosis is higher than on cytology alone (6).
Thoracotomy the above procedure can be performed when it is not possible to gain access to the pleural space because of bulky disease or loculation of the lung.
Emergency department: Under intravenous sedation and local anaesthetic, an ultrasound guided drainage of fluid might be performed.
Pericardiocentesis would be diagnosed and managed by a cardiothoracic surgeon, and/or interventional cardiologist after appropriate thoracic CT and cardiac imaging.
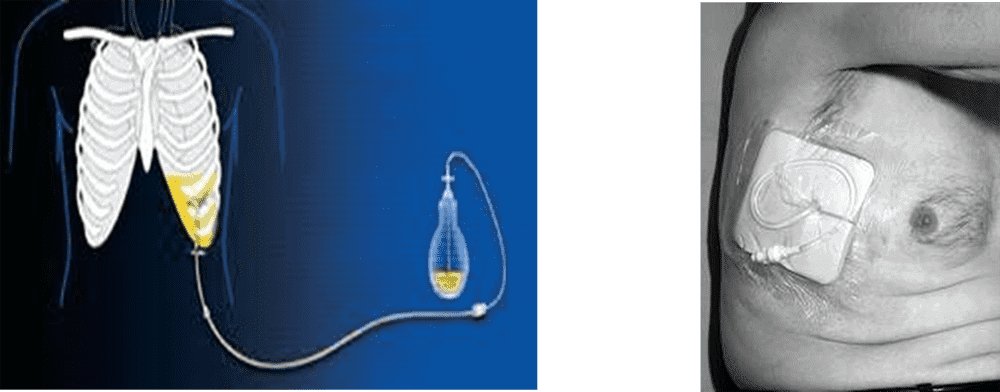
Indwelling pleural catheter (IPC)
It is always important to exclude other causes for SOB such as cardiac disease, infection, embolic disease, chronic obstructive pulmonary disease (COPD), asthma, asbestosis, and lung cancer.
Once a diagnosis is made, and if surgical options are not appropriate or available there is an additional method of managing the pleural effusion using a tunnelled indwelling pleural catheter (IPC). After the IPC has been inserted this system connects the patient to a vacuumed drainage system for intermittent drainage when symptoms become uncomfortable. Drainage can be done at a time and location convenient to the patient and performed by either themselves or a care provider.
The system can be inserted outside a major surgical service reducing the need for hospitalisation. For those who cannot access medical care easily, selfcare can provide some freedom of activity and quality living until such time as the tube can be removed or the patient comes to a comfortable end of life. In the absence of definitive drainage, IPC reduces the need for reliance on medical intervention for intermittent painful pleural taps.
The drain needs to be emptied when SOB escalates and can be on a needs basis or schedule, e.g., one, to three times per week. The need for regular emptying can restrict patient movement and travel. Obtaining a supply of sterile vacuumed bottles, storage of the bottles and the cost can be problematic, especially for people living in remote areas.
There is an emotional downside of the system on the patient and carer as the ever presence of a tube is a constant reminder of their disease and early end of life. On the other hand, whilst lung function may not improve, the rates of infection are low and in some situations the drain can be removed if a self-pleurodesis occurs. In Australia, the drains are commonly inserted by a cardiothoracic surgeon or experienced interventional radiologist.
There are two companies that market pleural drainage systems: Rocket (7) and Pleurx (8)
Independence Australia is a social enterprise based in Australia, providing choices and services for people living with a disability or other personal needs including pleural drainage systems (9).
2. Thoracic Pain
Thoracic pain on presentation can be indicative of aggressive tumour activity and/or advanced disease at the time of diagnosis. Pain should be treated according to the pain origin and medications can include a range of substances like simple oral analgesia, non-steroidal anti-inflammatory drugs (NSAID’s), narcotic medication, anti-neuropathic medications, and if malignancy is diagnosed then radiation therapy might be appropriate. Early referral to palliative care for symptom management can be advantageous to improve quality of life (QoL) (10). (See section Pain in mesothelioma)
3. Weight loss, decreased appetite
Weight loss and a decreased appetite are symptoms common to many illnesses and cancers, however in mesothelioma weight loss is more pronounced in patients with advanced disease.
4. Fatigue
Fatigue, to tire easily during exercise and the need to rest are also common and vague symptoms related to many other illnesses, however they are more pronounced in patients with advanced mesothelioma.
5. Night sweats
Sweats are a common symptom of many cancers. They are less likely for mesothelioma, but if so, they are more likely to occur at night (11).
How to manage sweats: There is no cure or treatment, however in the first place exclude an infective process in which case the use of NSAID’s like Paracetamol might lower a temperature through perspiration. Drug withdrawal can contribute to sweats so check that changes to a narcotic medication is not contributing. Sweats cannot be prevented so apply comfort care such as wearing loose clothing, placing a non-plastic layer between patient and bedding, ensure adequate supply of bedding to enable frequent changes, and enlisting help with laundry and care.
When Mesothelioma is Diagnosed
A diagnosis of mesothelioma elicits distressing thoughts and worries for the patient and family as some are quite bluntly told something like: “You have a terminal disease, there is no cure, you have months to live so sort your affairs.” This is commonly reported in support group meetings as a feeling of dejection, helplessness and being stripped of any hope to live long and enjoy family life (12). The aim of support is to assist patients to live a meaningful life by living as well as they can for as long as they can, either with or without medical treatment.
Access to appropriate support from the time of diagnosis is vital. Support can be in the form of clinical information, emotional and psychological counselling, and hearing how others have or are navigating the mesothelioma dilemma. Clinical information enables patients to explore and understand all treatment options, understand what is best for their individual situation, and empower the patient to make literal life and death decisions.
During the time of trying to understand the real impact of a mesothelioma diagnosis, sharing concerns and feelings with a trusted partner, carer, family member or trusted somebody is important.
Some practitioners talk about placing attention on the three A’s:
Attitude: stay positive but be realistic and surround yourself with positive people and support.
Appetite: eat healthy, fresh and basic nutritional food. If struggling with this see a dietitian.
Active: aim to maintain a good level of activity even during treatment. Doing a little exercise is better than doing nothing and when the patient least wants to exercise that is when it is most needed. A referral to an experienced Exercise Physiologist will be helpful.
The option to explore compensation
Depending on the legal entitlements of the country in which a person is exposed to asbestos some people who develop mesothelioma may be able to lodge a claim for compensation. Legal entitlements will vary between countries, and within countries, so it will be important to discuss this with appropriate governmental legislative legal officers.
Attending an asbestos victim support group can be beneficial to patients and their families as they can share information and emotional support from people who have been, or are in, the same situation.
Integrative Oncology and Supportive Care / Palliative Care
Opportunities to access treatment and the cost of treatment vary across the globe and even within countries. Unfortunately, all patients with mesothelioma will face a premature death and require optimal support to live well while they can and die with dignity. Traditionally, treatment involves using oncological therapy, interventional technology, or surgery to slow down disease activity, but combining these with integrative care and support, the impact of symptoms on ones’ wellbeing can be reduced and a sense of improved QoL can be achieved.
Integrative Oncology (13) combines supportive (14) and complimentary therapies like healthy nutrition, exercise physiology, mindfulness meditation, acupuncture, massage, dance, and palliative care with traditional medical therapy to provide ‘whole-person, patient-centred care’ that includes attention to psycho-social, emotional and spiritual concerns.
Decisions about treatment and supportive care need to consider the patient’s QoL by balancing the potential positive response and extension of life that might be gained from medical treatment against the potential adverse side effects, cost, and accessibility to that treatment.
How one makes a decision is likely to be based on the treatment availability, patient age, family social and financial circumstances, their ideology about end of life, their state of health and wellness, their desire to live longer, community preconceived ideas about treatments and outcomes, and many others.
1. Applying palliative medicine in mesothelioma
Mesothelioma is a devastating disease for patients and their families as it causes great suffering. For this reason, and because of the short median survival time of fewer than 12 months from diagnosis, it is important to introduce a palliative approach to patient management from an early stage, preferably from the time of diagnosis.
Palliative medicine aims to provide holistic care of people whose illness is acknowledged to be incurable. This approach combines three intentions:
the best possible treatment of physical symptoms
attention to and management of psychological and socio-emotional problems
support of the patient’s family during the illness and in bereavement
2. Symptoms in mesothelioma
Mesothelioma creates a particularly high symptom burden. It produces as much breathlessness and significantly more pain than lung cancer, as well as many other symptoms:
It is not appropriate to apply lung cancer care into mesothelioma because mesothelioma causes more dyspnoea and pain than lung cancer.
3. Steps to manage symptoms
Step 1: Understand the meaning of symptoms for individual patients
Step 2: Correct the correctable physical causes of symptoms
Step 3: Do all possible to reduce the perception of symptoms by using evidence-based treatments alongside attention to psychosocial factors
4. Breathlessness in Mesothelioma
Breathlessness is a very common symptom in MPM. Prevalence in mesothelioma is 96%, hence 21-90% in cancer.
The causes are:
Pleural effusion
Reduction in lung volume
Fixed lung
Pericardial effusion
Anaemia
Co-morbidities
Anxiety
Breathlessness can be terrifying to experience as shown by these quotes from patients:
‘Fighting for breath’, ‘gasping for air’, ‘drowning in fluid’, ‘suffocating to death’, ‘out of control’
Breathlessness is a bio-psychosocial phenomenon. Although they are hugely anxious, patients and relatives do not know when to call for help and often wait until they are desperate. Crises cause fear of imminent death. Breathlessness is visible, stigmatising and causes social isolation due to lack of mobility, loss of agency and embarrassment.
Note:
Breathlessness in mesothelioma has multiple aetiologies – not all physical
There is NO correlation between patients’ degrees of perception of breathlessness and blood gas levels or respiratory rate
There is NO correlation between relief of breathlessness and physiological measurements
Therefore, the only reliable measurement is self-report.
4.1 Management of Breathlessness
a) Treat all correctable causes, for example:
Aspirate pleural effusion and consider pleurodesis for recurrent cases*
Surgery may release a ‘trapped lung’
Surgical aspiration of pericardial effusion
Correct anaemia
Control heart failure
Antibiotic for infection
Explore and manage anxiety
* An indwelling pleural catheter (IPC) is effective in refractory cases in which pleurodesis has failed or cases where surgery is not an option. The indwelling drain can be managed by the patient’s family and may create pleurodesis with time. This has been found to reduce the number of hospital admissions for recurrent effusions (see Figure 1 and 2).
b) Everyone should have a hand-held fan
A hand-held fan is a simple low-cost, low-tech intervention that should be offered to every patient who has difficulty breathing; it will do no harm. The patient should direct the fan so that the cold air blows onto the lower part of the face. Hand-held fans are preferred to static fans, possibly because they promote a sense of mastery. The movement of cool air with a fan has been observed to reduce dyspnoea in patients. Stimulation of mechanoreceptors or temperature receptors mediated via the trigeminal nerve may alter afferent feedback to the brain and modify the perception of dyspnoea.
c) Use low-dose morphine
Suggested starting dose is 2.5mg oral morphine solution every 4 hours if needed to relieve breathlessness. If this fails to improve the patient’s breathlessness the dose should be increased gradually in line with the normal prescribing guidance for morphine.
Note:
The highest density of opioid receptors is found in alveoli, bronchi, and trachea. Morphine reduces minute ventilation by slowing respiratory rate and tidal volume. There is no evidence of respiratory depression when used in line with standard prescribing guidance for morphine.
d) Use complementary therapies such as relaxation, pacing activities, visualization to encourage the patient to gain some control.
e) Use rehabilitation or physiotherapy specialists to teach the patient about breathing control.
f) Educate carers so that they can assist the patient.
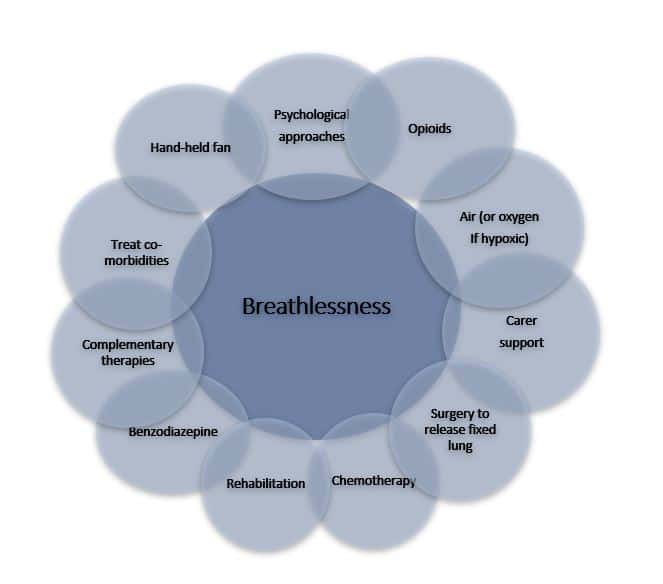
g) Use a multi-dimensional approach, considering all possible interventions as shown in the following diagram:
4-2. End of life terminal dyspnoea
This is extremely distressing for the patient and family. At end of life the following medications (or relevant medication as per country’s protocol) should be used to relieve distress:
IV morphine is choice: 2 – 5 mg IV Q5-10 minutes until relief
In rare cases, where relief is not obtained, it is ethical and compassionate to provide sedation by using barbiturates or benzodiazepines e.g., midazolam to relieve patient of symptoms (check country-specific regulations).
In summary, after correcting all treatable conditions, improve masterybefore breathlessness becomes refractory:
Pain score of mesothelioma is higher than the one of lung cancer (16).
Quote from patient with mesothelioma:
‘… the pain’s always there but I can control it with the medication, up to a point. It varies day by day; sometimes it’ll pull in my back, other times it’ll pull in my front, other times it’ll pull where I had my biopsy – it’s real
5.1 The cause of pain
Pain in mesothelioma is complex due to the various pain-sensitive structures that might be involved: the pleura, intercostal nerves, pericardium, diaphragm, ribs and vertebrae, spinal cord, and nerve roots plus nerve plexuses e.g., brachial plexus. Thus, the pain can be of inflammatory, neuropathic, or bony origin.
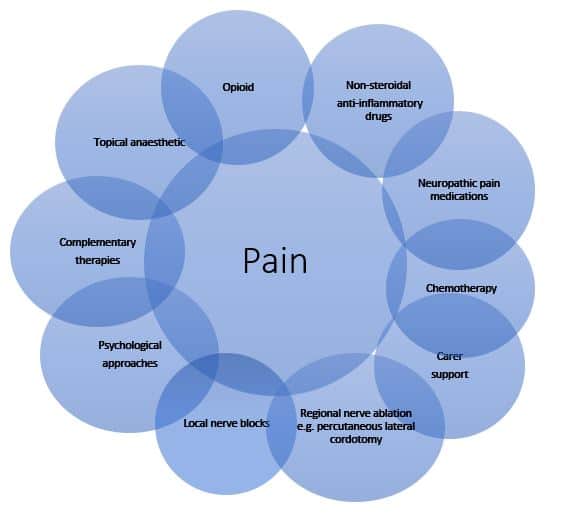
A combination of these types of pain frequently occurs and any perception of pain is greatly moderated by psychosocial factors. Fear and anticipation of pain are common to all cancers but the severe psychological burden in mesothelioma, and its impact on pain perception, requires particular understanding. Efforts to achieve pain control requires a multi-dimensional approach, see Figure 4.
Figure 4: Multidimensional interventions for pain
5.2 Management of pain in mesothelioma
Inflammatory pain: Tumour cells and possibly asbestos fibres invade soft tissues and interact with host macrophages release of cytokines, prostaglandins and other vasoactive substances which create the inflammatory response.
Treatment
This may respond to simple non-steroidal anti-inflammatory drugs (NSAIDs), or occasionally to corticosteroids (these may also increase appetite and general well-being but due to their side-effects are not recommended for long-term use). Regular paracetamol, 1gm qds or a mild opioid analgesic such as codeine may be added with benefit. Morphine is not very effective for this type of pain but more specialized drugs such as methadone and ketamine have anti-inflammatory actions.
Neuropathic pain: This arises when there is damage to either peripheral nerves or to nerve structures in the central nervous system. It can be self-perpetuating. Typical sensations that patients describe are burning or coldness, raw, ‘electric shocks’, numbness, itching and tingling. Hypersensitivity to stimuli (allodynia) and altered sensations (dysaesthesia) are common. Patients typically rub or tightly hold the affected area.
Treatment
Antidepressants e.g., amitriptyline, commencing at 25 mg at night
Anticonvulsants e.g., gabapentin
NMDA antagonists e.g., methadone (opioid) or ketamine
Topical lidocaine 5% patches for localized pain e.g., a small area on the chest wall or a track metastasis
Bone Pain: Local advanced tumour or metastatic hurt nerves in bone. Also, cytokines and koninis released by tumour cause long-term sensitisation as in neuropathic pain. This happens when rib and vertebral bodies are invaded by mesothelioma.
Treatment
Bone pain may have nociceptive, inflammatory, and neuropathic elements so any of the above medications may be useful. In addition, radiotherapy to a localised area of bone pain is highly effective.
Complications: rarely, paralysis of ipsilateral diaphragm, and 11% experience mild motor loss or dysaesthesia.
Breakthrough pain: This is pain that occurs between doses of a regular opioid and is not due to inadequate dosing.
Treatment
All patients who are prescribed sustained release morphine should have a supply of liquid oral morphine equivalent to 1/6th of the 24-hour dose to use if breakthrough pain occurs.
Example: A patient who is taking s/r morphine 60mg twice a day i.e.,120mg per 24 hours, should also have a supply of liquid oral morphine and take 20mg if breakthrough pain occurs. If more than 2 doses are required in 24 hours, then the regular long-acting dose of morphine should be increased to at least the sum of all doses required in the previous 24-hour period.
5.3 Pain control in mesothelioma – a suggested model
Step1:Non-opioid +/- NSAIDs
For localized chest wall pain consider topical local anaesthetic or, if bone pain, use radiotherapy.
Step 2:Start opioid
Use short-acting oral morphine solution initially and start at low dose e.g., 2.5mg 4-hourly as required. Once pain control has been achieved, usually within a few days, convert the effective total 24-hour dose into regular doses of a long-acting morphine – to be taken regularly. A laxative should ALWAYS be prescribed with morphine as intractable constipation is a very distressing side-effect. Sometimes patients cannot tolerate the side effects of morphine in which case an alternative opioid such as oxycodone may be used.
Step 3: Add a neuropathic pain agent
If any clinical features suggest neuropathic pain and there has been no improvement on morphine, then stop morphine and commence a neuropathic pain agent (see above). If morphine has helped but there are still features of neuropathic pain, then add a neuropathic pain agent as above. In some cases, two neuropathic pain agents with different modes of action may be more effective than one.
Step 4: Refer for Specialised interventions
If distressing pain persists, refer quickly for specialised interventions:
Ketamine and methadone: These 2 analgesic medications can be highly effective in refractory pain, but both require specialist management due to their complex actions and the possibility of major side effects.
Percutaneous cervical cordotomy: This technique involves ablation of the contra-lateral lateral spinothalamic tract and is used for unilateral severe pain below the clavicle. It can be very useful in pleural mesothelioma. The patient must be able to lie still for 1 hour and be conscious and cooperative – 47% achieve prolonged benefit (17). This is only available in specialised centres.
5.4 Pain assessment
The rule is that ‘pain is what the patient says it is’ – therefore self-assessment is the only reliable method of pain evaluation. Pain score charts or visual analogue scales can be extremely useful in determining whether or not treatments are effective when used by individual patients as a self-comparison method.
5.5 How to use morphine
Start low dose every 4 hours, using liquid oral morphine
Increase quickly – every 3 days initially – until pain is controlled
Then switch to a sustained release preparation
If side effects occur, consider:
Is the dose too high?
Would an alternative opioid be better? or,
Ask ‘Is this neuropathic pain?’ If so, change to medication for neuropathic pain.
Other Opioid: Oxycodone, fentanyl, methadone, KetamineWould an alternative opioid be better? or,
6. Suggestions for managing other common symptoms
Cough – establish cause; consider dexamethasone if an inflammatory cause, gabapentin if muscle spasm, antibiotic if infection. Rarely, after radical extra-pleural pneumonectomy (EPP), consider post-surgical bronchial fistula.
Sweating – consider cimetidine, use cotton clothing and a fan.
Fatigue – may benefit from rehabilitation if well enough, pacing of activities or corticosteroid (short-term).
Nausea – metoclopramide or haloperidol initially but may need corticosteroid +/- levomepromazine. Two thirds of patients need more than one anti-emetic in combination.
Anxiety – honest but compassionate information and assurance of continuing support for the patient and family. If the patient is also depressed, mirtazapine is particularly useful due to its side effect of increasing appetite as well as lifting mood. Complementary therapies may help e.g., visualization and relaxation. Patients who are still well enough can benefit from attending an asbestos victim support group, if available in their country. In some cases, formal psychiatric assessment may be necessary. Consider involvement of faith leaders if appropriate.
7. Summary: For best practice palliative care in mesothelioma
Address all symptoms that cause suffering
Pain in mesothelioma is complex and severe, breathlessness is terrifying, multiple other symptoms occur, and psychological issues worsen the experience of symptoms. Multiple medications are often required.
Act quickly
The British Thoracic Society guidelines suggest palliative care by specialists should be introduced in the early stages of mesothelioma (18). However even in the UK around half the mesothelioma patients do not receive palliative care. Severe symptoms arise quickly in mesothelioma and tend to get worse as the disease progresses (unlike in most cancers where they tend to plateau). Act quickly and refer rapidly for appropriate treatment by a palliative or pain management specialist working within a multi-disciplinary team.
Address psychosocial issues
Mesothelioma causes much distress, and the psychosocial issues exacerbate physical problems. Understand what is causing distress to individual patients, always treat them with respect and compassion, and reassure them that you will support them and their families throughout the illness.
Medical Oncology
1. Standard chemotherapy
The standard chemotherapy drugs for pleural mesothelioma are pemetrexed in combination with cisplatin or carboplatin. Research shows this combination can improve quality of life (QoL) and increase survival by a few months more than using a single drug (19).
The goals of chemotherapy are to increase length of life, to shrink the cancer, reduce symptoms and improve QoL. However, chemotherapy does not work for some people.
Further information:
Chemotherapy for pleural mesothelioma (20)
Understanding chemotherapy (21)
2. Immunotherapy
Immunotherapy is a type of drug treatment that uses the body’s own immune system to fight cancer. It is different to chemotherapy, which works by killing cancer cells. Different types of immunotherapy work in different ways. Some stimulate the immune system, so it works better against cancer. Others remove barriers that stop the immune system attacking the cancer. Checkpoint immunotherapy is currently available in Australia for some types of cancer. The role of immunotherapy in treating mesothelioma is still being investigated but it has worked well for some people and has not helped others.
Further information:
Immunotherapy (22)
Understanding Immunotherapy. A guide for people affected by cancer (23)
3. Clinical trials
Clinical trials are research investigations in which people volunteer to test new treatments, interventions, or tests to prevent, detect, treat, or manage various diseases or medical conditions. Some investigations look at how people respond to a new intervention and what side effects might occur. This helps to determine if a new intervention works, if it is safe, and if it is better than the interventions that are already available.
Clinical trials might also compare existing interventions, test new ways to use or combine existing interventions or observe how people respond to other factors that might affect their health (such as dietary changes).
The World Health Organization (WHO) definition for a clinical trial is:
‘Any research study that prospectively assigns human participants or groups of humans to one or more health-related interventions to evaluate the effects on health outcomes’
Clinical trial interventions include but are not restricted to:
experimental drugs
cells and other biological products
vaccines
medical devices
surgical and other medical treatments and procedures
psychotherapeutic and behavioural therapies
health service changes
preventive care strategies and
educational interventions.
Researchers may also conduct clinical trials to evaluate diagnostic or screening tests and new ways to detect and treat disease (24).
4. Factsheets – Management of side effects of chemotherapy treatment
Radiotherapy is a cancer treatment that uses a controlled dose of radiation to kill or injure cancer cells, slow tumour growth, and hopefully cause tumour shrinkage, reduce symptoms and associated discomfort. The role of radiotherapy in treating mesothelioma is limited because mesothelioma cells are not highly sensitive to radioactive waves and therefore have a poor response to this treatment; and the dose required for effect is too toxic. Radiotherapy can offer some relief to pain where a specific area can be targeted. However, radiotherapy can cause skin changes because it can damage healthy skin cells in the treated area.
The consultation process is similar to any other cancer: Initial consultation-> Simulation-> Planning-> Treatment->Follow-up.
There are two common techniques used to perform lung surgery for mesothelioma. The most frequent today is video assisted thoracoscopy or VAT with some surgeons offering thoracotomy (open surgery) when appropriate. Both procedures enable a partial pleurectomy and decortication as well as talc pleurodesis.
A third option is radical surgery as part of trimodality therapy aiming to remove all macroscopic and microscopic tumour. This treatment is only offered inside a specialised mesothelioma oncology service where there is an experienced cardiothoracic surgeon within a specialized cardiothoracic service.
1. Video Assisted Thoracoscopy (VAT) (keyhole surgery)
Several small incisions (called port holes) are made in the side of the chest to allow a small camera and instruments to be passed into the chest. The surgery is performed via these port holes.
This procedure allows for optimal biopsy specimen, direct visualisation of disease present and corrective action such as pleurectomy and decortication. When lung tissue cannot fully expand it is usually because of prolonged collapse related to fluid, infection, or bulky tumour growth. The chest wall and pleura, can be partially stripped, called pleurectomy, along with the lung pleura being surgically peeled away called decortication. The lung is then able to re-expand and fuse the lung and chest wall creating a surgical pleurodesis.
2. Thoracotomy (open surgery)
The chest cavity is entered via an incision on the back of the chest approximately 15-25 centimetres long. The ribs are spread to allow entry into the pleural space for partial pleurectomy and decortication (p/d). This procedure enables better access to debulk tumour that has been constricting lung expansion. Prior to VATs being perfected in the 1990’s open thoracotomy was standard mesothelioma surgery.
2.1 Talc pleurodesis
A talc pleurodesis is a procedure whereby sterile talc powder is instilled into the pleural space. The aim of this procedure is for the talc to cause inflammation between the two membranes that surround the lung and chest wall – the visceral and parietal pleura. The two pleura adhere to each other so that the lung will not collapse, and the fluid cannot be produced to collect in the pleural space. Talc pleurodesis is standard for both VAT and open surgery. In some expert centres it is offered by interventional respiratory physicians.
2.2 Postoperative care after lung surgery
The important issues for a good recovery are:
Pain relief: Ensure an effective pain management regime is initiated beginning in the recovery room to enable patient mobility and optimal respiratory function.
Physiotherapy: Initiate regular professional and self-physio to ensure optimal respiratory function and adequate functional recovery.
Nutrition: Eat a well-balanced diet to aid healing and recovery.
Prevention of constipation: Aperient medications should be prescribed and taken in conjunction with narcotic medications to prevent constipation.
3. Radical surgery: Extra Pleural Pneumonectomy (EPP) as part of trimodality therapy
There are a small number of people diagnosed with pleural mesothelioma as an incidental finding or are found to have minimal disease. They also have few co-morbidities, are fit and well and young enough to be considered for radical therapy. In Australia this is offered as trimodality therapy.
Trimodality therapy comprises of three sequential treatments. It begins with induction chemotherapy consisting of three cycles of standard chemotherapy, followed by radical cytoreductive surgery to remove the complete lung, and chest pleura of the affected lung called extra pleural pneumonectomy (EPP). This is followed by six weeks of radical radiotherapy. The Sydney Cancer Centre is the only centre in Australia that has an established treatment programme and has published results (39).
The best way to treat mesothelioma is still a research mystery. The role of trimodality therapy continues be a topic of debate in the professional mesothelioma community, however there are a small number of long-term survivors (up to 15 years) after EPP in Australia. Patients can live with greater QoL after enduring the three-stage treatment regime spanning nine months.
The QoL of patients, carers and families living with mesothelioma has focused on outcomes related to oncological treatment rather than the lived experience (16, 42, 43). However, an Australian study by Warby et al. (44) explored the patient and caregiver experience of living with mesothelioma using interviews to collect data and concluded that: “Satisfaction with treatment was high, but participants identified need for improved communication and quality information, discussion about all treatments, end-of-life assistance, and caregiver support after the patient’s death.”
A Japanese study led by Nagamatsu et al. (45) concluding that “Survivors of MPM have impaired function, experience a variety of symptoms, and have a lower QoL.(45) The duration of disease and a poor performance status (PS) correlated with impaired QoL. Survivors of MPM, even those in good physical condition, need broader support.”
The psychological impact of a mesothelioma diagnosis on the patient and family is understudied, however it is recognised that patients experience many negative emotions such as depression, fear, anxiety, hopelessness, guilt, shame, and rage (10, 46, 47).
The powerful emotions of loss and grief are experienced by both patient and family during the mesothelioma journey, beginning at the diagnosis and then intermittently throughout the journey and continuing after the death. They are commonly a consequence of the unexpected premature death and associated losses, such as: loss of control over one’s health and life, loss of well-being, loss of the ability to continue employment and associated financial implications, loss of friends and shared memories, loss of a partner, parent, or sibling, being responsible for increased burden on others.
Grief on the other hand is an expected response, that can elicit physical and emotional responses that need to be recognised as normal and real. How one reacts to loss and grief varies and personal reaction can shape and impact individual long-term coping mechanisms.
It is vital that patients and families are offered psychological support, know how to reach out for support, and health professionals are alert to abnormal signs of loss and grief to avoid serious mental health problems (48).
A very recent, but limited, UK study by Sherborne et al. (49), demonstrated that the effects of living with mesothelioma on patients and carers resulted in both complex and inter-relating psychology that requires in depth study.
Comprehensive Quality of Life Outcome questionnaire (CoQoLo) (51)
Functional Assessment of Cancer Therapy: General (FACT-G) (52) (53)
Patient and Family Support
Patient and family support for anyone diagnosed with pleural mesothelioma is an essential part of care but sadly it is often the last consideration in health care funding. This should not be the case when a new disease is evolving, and services are being developed. Common cancer groups in some high-income countries have specialist trained nurses to provide care and support. This should be the case for mesothelioma as the symptom burden and need for medical and emotional support is high (5).
1. Function and aims of support
The aim of support is to help the patient with mesothelioma live as well as they can for as long as they can with quality. To enable this, they need to be empowered with information to help them understand the disease, diagnosis, prognosis, and treatment options. Information will also help them evaluate their life priorities when making decisions and choices about accepting treatment or otherwise.
In Australia, this support is provided from two sources:
hospital and community health professionals providing evidence-based information and clinical support, and
patient advocacy support organisations.
2. Hospital & community health professionals providing evidence-based information & clinical support
It was implied above that information helps to empower patients to make informed decisions but where do patients get that information from? Mesothelioma is a rare disease; low patient numbers means there is little clinical experience for all health practitioners. Additionally, there is limited access to formal nurse education and minimal attention given to learning about ARDs in medical training curriculums. In international cancer care circles, specialist cancer nurses play an integral part in providing cancer care and support. In countries where there are more cases per annum like the USA (around 3000), UK (2,700) and Japan (around 1500) (54) there are funded specialist mesothelioma nurses who attend formal training programmes (55-57).
In Australia there is between 700 and 800 cases of mesothelioma per year (58) and New Zealand around 150 cases per year (59) , patients are supported in the hospital and community system by the available small number of lung cancer nurse specialists. Mesothelioma patients in Australia, receive clinical care from general oncology and surgical cancer nurses, and more specialised care and coordination is provided by the small number of lung cancer nurses across the country.
Since 2014 the Asbestos Diseases Research Institute (ADRI) has provided a dedicated Mesothelioma Support Service. This is a nurse led evidence-based support service that has evolved in response to the reported unmet needs of patients and carers (44). The service is provided by two post graduate qualified registered nurses experienced in mesothelioma care and issues who help the patient interpret and understand information they have received about the diagnosis, prognosis, and treatment options. They help patients navigate a complex health care system; a system that often has little understanding of the disease they are living with. The support provided by these nurses ranges from beginning through to advanced information, advice and guidance through treatment and supportive / palliative care, ultimately ensuring the patient and family are adequately prepared for a dignified end to life.
Further reading:
Unmet needs and future outlook of mesothelioma management. (60)
The lived experience of patients with pleural mesothelioma (61)
‘Hands of Time’: the experience of establishing a support group for people affected by mesothelioma. (62)
Understanding the palliative care needs and experiences of people with mesothelioma and their family carers. (63)
Recommendations for improving follow-up care for patients with mesothelioma: (64)
3. Who needs support?
Anyone diagnosed with mesothelioma needs support however the ADRI Mesothelioma Support Service has identified three specific groups:
those receiving integrative oncology and supportive palliative care,
those who have had radical treatment with extra pleural pneumonectomy (EPP), and
the bereaved struggling with grief and loss.
Within groups 1 and 2 there are three subcategories:
patients who are newly diagnosed and want clinical information and empathetic support,
patients in a stable condition, who want to live a ‘normal’ life for as long as possible,
and patients with progressive (symptomatic) disease with complex medical and psychological needs.
Contact with patients’ can be at any point along a timeline from diagnosis but early contact is ideal. Modern technology has opened the world of communication so that even those living in remote locations can be connected and elderly patients who may not use IT can be connected by telephone. However, a connection cannot happen without a referral to a support service. Just as awareness about asbestos exposure can lead to an earlier diagnosis, early referral and access to a support service is likely to have a positive impact on the experience of a patient living with mesothelioma.
The ADRI support service provides contact and support via telephone, email, teleconferencing, face to face support groups and special events.
4. Types of contact
Telephone calls
Telephone contact is the key method of communication providing a link for the patient to the clinical and research world. Patients (and carers) need and want to know they can reach an experienced person to help them clarify and understand the clinical information and advice. They have the opportunity to discuss concerns they may have and know there is someone who comprehends what they are hearing, feeling, and living through.
Teleconferencing
During COVID-19, teleconferencing provided group communication and maintained connections between those living with similar experiences, thereby helping to reduce the isolating impact of COVID-19, distance, and rarity of the disease. Whilst Zoom/videoconference meetings were an option, there are people who do not have IT skills or smart phones, so teleconferencing ensured all people had equal opportunity to participate.
Video conferencing
The small number of people taking up the opportunity of video conferencing has resulted in more focused and concentrated conversations that have been especially beneficial to newly diagnosed families eager to feel some optimism about living with mesothelioma.
Email
Email supports communication when telephone contact is not successful. Emails share information about support group meetings and other activities. Most importantly, it allows for the dissemination of new and updated clinical information, research findings, and available clinical trials.
Support groups
The ADRI service facilitates face to face support group meetings that have a clinical and educational focus. The group meetings are targeted to a specific mesothelioma population in Australia. Some meetings have guest speakers addressing a specific topic on mesothelioma management from diagnosis to bereavement or topics according to support members preferences.
Research conducted by Cancer Council NSW has shown that people participating in support groups have lower levels of anxiety and depression than those who don’t (65) and identify the reasons people choose to join and stay in a support group as:
The sense of belonging and of being supported
People can often feel isolated and unsupported when they are diagnosed with cancer. By joining a support group people can develop a sense of belonging and feel comfortable enough to share their feelings with people who have had similar experiences. Groups develop a sense of community, and this can assist with the psychological effects of cancer and may improve their ability to cope. Many people who join support groups find that they give as much as they receive, which raises their confidence and their ability to cope.
Feeling safe
Inside a support group people feel protected and safe to express their feelings. It is often the case that people must hide their feelings outside of the group to protect others.
Feeling empowered
People join support groups to not only look for encouragement and optimism but for inspiration, hope for survival and QoL. Many support groups provide access to a range of highly qualified speakers. Although many speakers will be health professionals, many other people can contribute to the group such as artists, writers, yoga instructors, massage therapists. By joining a support group people can feel empowered through their increased knowledge and understanding of cancer, research, and treatments.
A place to relax
Support groups provide a safe place for people to relax and be at ease with others who understand what they are going through. They can also allow an environment where people can feel comfortable to cry, laugh and joke – and just be themselves!
Coming to a first group meeting can be an enormous challenge for patients’, carers, and families as they are fearful of what they might hear and see, especially in the context that they may have been given poor prognostic information at the time of diagnosis. Through telephone and email contact there is a shared trust between patient and professional so that attending a meeting provides continuity of support and care, builds patient confidence whilst at the same time helps break the negative barrier that the patient imagines but in reality, may not experience. The frequency of a group depends on the needs of those within the group and geographic locations. Many are monthly or every second month at a time and location that suits needs and cost. The ADRI Mesothelioma Support Service believes informal time to chat over food is important for networking.
It is common for people to move between support groups as their need for information changes. The ADRI Mesothelioma Support Service provides support to four specific group of people:
A general group for any patient living with mesothelioma,
A group for patients who have had radical treatment called the Well Living EPP group,
A group for patients with peritoneal mesothelioma; and
For the bereaved of either of the previous groups.
It is also common to have mixed groups of patients and bereaved. For example, those who become bereaved may also feel comfortable in a general or EPP group because of the prior confidence and friendships that may have developed. Likewise, they too can use their knowledge and experience to give back to those who are currently living a mesothelioma journey. A mixed group does require careful management of changing dynamics hence the need for a facilitator who will be alert to and aware of sensitive situations.
5. Other activities
The ADRI Mesothelioma Support Service holds three special activities each year:
An annual walk to raise awareness about the issue of asbestos. The 4-kilometre walk recognises the patient who is living with mesothelioma, acknowledges the families who have lost a loved one and raises public awareness about the dangers of asbestos in the built environment.
An annual education session that addresses a specific issue related to the needs of mesothelioma patients. Closed group webinar meetings have proven to be useful in terms of time and as an educational resource for new patients and families to view (66) (67).
Record patient conversation material so ongoing calls are appropriate and timely. Strict government standards regarding privacy and the secure storage of patient health information must be followed to protect information from unauthorised access, loss, or other misuse.
Role of Supporting Organisations
Overview of support organisations
In many developed countries the 1960s to the 1970s was the height of asbestos manufacturing and use, with the medical profession, health and safety regulators, industries and governments becoming aware of the dangers of asbestos. At that time there were a few campaigners and organisation willing to confront the large asbestos producing companies. The asbestos support groups evolved from the early work of those who campaigned vigorously for the rights of those who were suffering from ARDs.
The support organisations grew out of a common concern for victims of ARDs and to take a united action to further the interests of victims to obtain compensation. These organisations included members from trade unions, lawyers, benefit advisors, occupational health and safety organisations and victims of ARDs and their families.
Typically, support organisations are community-based; comprising of a committed volunteer base of family members affected by ARDs and a small cohort of paid staff with a high level of collaboration with other organisations from other sectors. Their aim was to raise awareness of the injustice and suffering experienced by this group and to address the unmet needs for advice and support.
This overview of support organisation from around the world is based on the information that appears online and cannot completely describe the breadth and depth of the work carried out in the different communities nor the passion behind these support organisations.
Support organisations serve as an advocacy group that provides hope and delivers quality information and resources to patients with ARDs and their families. They provide free access to services, support, guidance, and information to cope with ARDs so that they may live well for longer with their loved ones. The support organisations are independent (however many are sponsored by law firms or supported by unions) caring, not-for-profit, charitable organisations founded to pursue the following broad objectives in asbestos related issues:
Key functions of support organisations provide:
Services – free counselling and support services to those who have developed ARD and their families and the bereaved, those who have lost someone to ARDs.
Resources – providing information on the latest medical and scientific research on ARDs and raising community awareness of the dangers associated with asbestos.
Events – fundraising for medical research and support services for asbestos diseases patients and their families
Advocacy / Campaigns – lobbying and providing advocacy in asbestos-related matters including medico/legal matters (Workers’ compensation/common law) and industrial and environmental hygiene.
1. Services
The services provided by the support organisations aim to ensure that all those affected by ARDs have access to information, advice, help and ‘practical, social and emotional’ support.
Many organisations offer peer-to-peer support through a telephone service providing a vital communication link between the patient, family and the bereaved. The empathic and supportive listener can provide information and advice about diagnosis, treatment, compensation, legal and financial help as well as emotional support.
The sharing of experiences with other people who have also been affected by ARDs cannot be underestimated. Social isolation is a key factor when caring for someone with an ARD whilst peer-to-peer support is the mainstay of these services it is often provided through a variety of means including online support groups and Facebook. These online services also help to keep in contact and support people living in regional or remote communities where there is often a lack of transport to specialist care and in some communities, there can be a fear and distrust of services or a lack of culturally safe support.
Many of the support organisations provide advice on compensation entitlements to encourage the victims and the families so that any benefit received may help to improve their QoL. This will often entail access or referral to legal services.
2. Resources
Most support organisations provide online resource through their websites about the dangers associated with asbestos. They will also provide information about ARDs that is easily understood in several languages to limit any language and health literacy barrier with the latest medical information. Many of these group regularly communicate with experts for specialist advice where they do not have the professional experience or resources to deal with issues.
The support organisations engage in strategies to ameliorate ARDs including raising awareness of the dangers of asbestos and education programmes. They will frequently provide the following information on their websites and in printed material:
Asbestos information
History of asbestos
The different forms, including naturally occurring asbestos (NOA). This information often includes a full description, the types of asbestos with accompanying photographs.
Asbestos awareness
To raise awareness of the dangers of asbestos and to reduce further exposure many of these organisations describe on their websites why asbestos is dangerous, where it can be found, what materials contain asbestos, how it can be removed safely, how to deal with it and how to dispose of it correctly.
In developed countries traditionally most of the ARD cases were occupationally related and therefore many of the support organisations provided information around the workplace to raise awareness of the dangers of asbestos amongst targeted communities such as tradespeople. Their websites provide information on how to handle asbestos in the workplace and guides for various profession such as electricians, builders, plumbers, tilers, etc.
Education Programs
As part of the asbestos awareness campaign several support organisations run educational training programs to raise the awareness of the dangers of asbestos. These training programs are often carried out in conjunction with statutory authorities, government departments, community, and workplace groups. The resources provided include face to face educational programs, videos, and the support of medical research through scholarships/donations. These training programs enable the delivery and evaluation of an asbestos awareness program within the wider community and have the added value for people affected by ARDs by providing positive life affirming action.
Examples of these educational training programs are:
Technical and Further Education (TAFE) courses for: carpenters, plumbers, electricians, engineers, etc.
University students –medical, nursing, biomedical research, and environmental sciences
Local councils – council based to enable the delivery and evaluation of an asbestos-awareness raising program within the wider community.
Workplace groups, community groups (State Emergency Service volunteers), hardware stores or building and home improvement shows, local field days and club meetings, etc.
ACM Registers
Asbestos-containing materials (ACMs) remains in society as it was used in over 3,000 products in the construction industry, manufacturing, and chemical refining during the 20th century. It can be found in wall and roof sheeting, insulation and flooring, brake linings and gaskets. It has been estimated that one in three houses in Australia built or renovated before 1989 contains asbestos. Exposure to asbestos within this built environment, particularly during home renovations and repairs, has resulted in a new wave of environmental and non-occupational exposures of ARDs. To combat this new wave, many of the support organisations collaborate with the wider community to provide information specifically for homeowners, with such topic as:
safety for homeowners
guides for minor renovations
guides for your neighbours
guides for rental properties
As there are so many products containing asbestos many of the support organisations will provide a register of ACMs. These registers can be very comprehensive providing a description, background history and information of the ACM on when and where it was produced, where and how it was used, with accompanying photographs and references.
As a large amount of ACM’s remain in the built environment, they then become a major issue during adverse events and natural disasters such a storms or fires. Therefore, many support organisation will provide information on how to handle asbestos after a natural disaster or in fire damaged buildings.
In many developed countries there are regulations regarding removing and disposing of asbestos and can impose large fines and serious penalties to those who violate the laws around asbestos. To reduce the risk of exposure and to safeguard workers and the public, the support organisation encourage people to dispose of ACM’s properly and will provide information on current asbestos legislation, accredited testing and licensed removal and disposal companies.
Asbestos-related diseases (ARDs)
All support organisations provide information on ARDs which can appear on their website or provided in a booklet. Some of the information is reviewed by the top mesothelioma specialists in each of the various countries. Some organisations keep up to date with the latest medical and scientific developments associated with ARDs. They will include information on asbestosis, pleural plaques, mesothelioma, and lung cancer with associate information and resources, depending on the disease.
Other resources and links
Not all patients with ARDs live in the cities and will often have to travel to major centres for appointments with specialists and treatment which can then delay a diagnosis. The additional stress associated with travel can be alleviated with support from the victim organisations with travel and accommodation. Some organisations have an outreach program connecting patients with the best care based on their location to build relationships and discuss current and emerging treatment options with doctors and researchers. Barriers to effective health care is not only include the tyranny of distance but also socioeconomic factors and often support organisations will have medical loan schemes for assistive equipment such as humidifier, nebulizers, member discount on oxygen; oxygen concentrators, oxygen bottles and wheelchair or provide information to access Government and community support services.
3. Events
Many of the organisations run events to provide face-to-face empathic support meetings for patients and their families, to raise awareness of the dangers of asbestos and to fundraiser.
Meetings
The support organisation will conduct regular meetings often across different locations to ensure all those affected by ARDs have access to help, information, advice, and support. These meeting are not only informative, provide empathic support to patients and their families, but also provide an opportunity, usually on a volunteer basis, for people affected by ARDs to positively give back to their community by supporting others. As well as the regular meetings they may conduct excursions to places of interest or to celebrate special commemorative days. The support organisations will often run seminars or symposiums hosted by medical research institutes, law firms or NGOs to update their members on the latest medical and legal information.
Awareness
National asbestos awareness campaigns are held around the world on various days, the date is often important to that nation, such as when asbestos was banned. These campaigns can range from a day to a month with a targeted asbestos awareness campaign such on homeowners who are undertaking renovation or demolition. National asbestos awareness will often incorporate mesothelioma action or a memorial day to remember those who have lost their lives to ARDs.
Fundraising
To support research into ARDs and to enhance the capacity of ongoing supportive services the organisations undertake a range of fundraising activities, which can include a walk for mesothelioma, golf days, race days, gala dinners, raffles, and merchandise such a wristbands, to help raise awareness of the dangers of asbestos and show support for those it has impacted. These fundraising events are often sponsored by local businesses or law firms.
Advocacy
The support organization advocate for victims of ARDs and campaign for social justice and compensation. These activities include:
provide opinion and lobby government including the banning the import and use of asbestos and obtaining equitable treatment.
participate in local, national, worldwide issues regarding asbestos including making representation at international meeting such as the Rotterdam Convention relating to chrysotile.
represent the organization on government initiatives such as Strategic Plan for the Safe Management of Asbestos.
make public statements (media releases, news items) with respect to the plight of victims and the dangers of asbestos exposure
assist patients to explore their legal options in obtaining compensation for those who qualify
Support Organizations
Australia
Asbestos Council of Victoria / Gippsland Asbestos Related Diseases Support Inc (ACV/GARDS)
www.gards.org
Asbestos Disease Support Society (ADSS)
www.adss.org.au/asbestos-diseases/
Asbestos Diseases Foundation of Australia (ADFA)
www.adfa.org.au
Asbestos Diseases Society of Australia Inc (ADSA)
www.asbestosdiseases.org.au
Asbestos Diseases Society of South Australia Inc (ADSSA)
www.adssa.org.au
Asbestos Free Tasmania Foundation (AFTF)
www.asbestosfreetasmania.org.au
Asbestos Victims Association (South Australia) Inc (AVA)
www.avasa.au
Asbestosis & Mesothelioma Association of Australia (AMAA)
www.asbestosassociation.com.au
Reflections through Reality
www.reflections.org.au
Brazil
ABREA
www.abrea.org.br
Bahia Association of Asbestos Exposed – ABEA
http://abeacontraoamianto.blogspot.com.au/
Canada
AREA Fund
http://www.areafund.ca
England
Cheshire Asbestos Victims Support Group (CAVSG)
http://www.cavsg.co.uk
Cumbria & Lancashire Asbestos Support Advice Group (CLASAG)
Japan Association of Mesothelioma and ARD Victims and their Families
https://www.chuuhishu-family.net/english/
Scotland
Clydebank Asbestos Group
www.clydebankasbestos.org
Clydeside Action on Asbestos
http://www.clydesideactiononasbestos.org.uk
Switzerland
Verein für Asbestopfer und Angehörige
http://www.asbestopfer.ch/
United States of America
Asbestos.com
www.asbestos.com
Asbestos Disease Awareness Organization (ADAO)
http://www.asbestosdiseaseawareness.org
Mesothelioma.com
www.mesothelioma.com
Mesothelioma Applied Research Foundation
www.curemeso.org
Mesothelioma Guide
www.mesotheliomaguide.com
Mesothelioma Prognosis Network
https://www.mesotheliomaprognosis.com/
Further information:
Understanding asbestos support and services in Australia. (69)
Asbestos Support Group Network (70)
References
Mothoneos J, editor. Understanding Mesothelioma. A guide for people with cancer, their families and friends.: Cancer Council Australia; 2019.
Milano MT, Zhang H. Malignant pleural mesothelioma: a population-based study of survival. J Thorac Oncol. 2010;5(11):1841-8.
Musk AW, Olsen N, Alfonso H, Reid A, Mina R, Franklin P, et al. Predicting survival in malignant mesothelioma. Eur Respir J. 2011;38(6):1420-4.
Bibby AC, Dorn P, Psallidas I, Porcel JM, Janssen J, Froudarakis M, et al. ERS/EACTS statement on the management of malignant pleural effusions. Eur J Cardiothorac Surg. 2019;55(1):116-32.
Guidelines for the Diagnosis and Treatment of Malignant Pleural Mesothelioma Asbestos Diseases Research Institute; 2013. 112 p.
Gelzinis TA. The 2019 ERS/ESTS/EACTS/ESTRO Guidelines on the Management of Patients With Malignant Pleural Mesothelioma. J Cardiothorac Vasc Anesth. 2020.
Hoon SN, Lawrie I, Qi C, Rahman N, Maskell N, Forbes K, et al. Symptom Burden and Unmet Needs in MPM: Exploratory Analyses From the RESPECT-Meso Study. J Palliat Care. 2020:825859720948975.
Arber A, Spencer L. ‘It’s all bad news’: the first 3 months following a diagnosis of malignant pleural mesothelioma. Psychooncology. 2013;22(7):1528-33.
Seely DM, Weeks LC, Young S. A systematic review of integrative oncology programs. Curr Oncol. 2012;19(6):e436-61.
Clayson H. The Experience of Mesothelioma in Northern England. University of Sheffield: University of Sheffield; 2007.
Nowak AK, Stockler MR, Byrne MJ. Assessing quality of life during chemotherapy for pleural mesothelioma: feasibility, validity, and results of using the European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire and Lung Cancer Module. J Clin Oncol. 2004;22(15):3172-80.
Jackson MB, Pounder D, Price C, Matthews AW, Neville E. Percutaneous cervical cordotomy for the control of pain in patients with pleural mesothelioma. Thorax. 1999;54(3):238-41.
Woolhouse I, Bishop L, Darlison L, De Fonseka D, Edey A, Edwards J, et al. British Thoracic Society Guideline for the investigation and management of malignant pleural mesothelioma. Thorax. 2018;73(Suppl 1):i1-i30.
Vogelzang NJ, Rusthoven JJ, Symanowski J, Denham C, Kaukel E, Ruffie P, et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol. 2003;21(14):2636-44.
Yan TD, Cao CQ, Boyer M, Tin MM, Kennedy C, McLean J, et al. Improving survival results after surgical management of malignant pleural mesothelioma: an Australian institution experience. Ann Thorac Cardiovasc Surg. 2011;17(3):243-9.
McLean J, McCaughan BC. Diagnosis and treatment: the journey of a petient with malignant pleural mesothelioma. Sydney: The Baird Institute; 2013. 79 p.
Schwartz RM, Watson A, Wolf A, Flores R, Taioli E. The impact of surgical approach on quality of life for pleural malignant mesothelioma. Ann Transl Med. 2017;5(11):230.
Arnold DT, Hooper CE, Morley A, White P, Lyburn ID, Searle J, et al. The effect of chemotherapy on health-related quality of life in mesothelioma: results from the SWAMP trial. Br J Cancer. 2015;112(7):1183-9.
Warby A, Dhillon HM, Kao S, Vardy JL. A survey of patient and caregiver experience with malignant pleural mesothelioma. Support Care Cancer. 2019;27(12):4675-86.
Nagamatsu Y, Oze I, Aoe K, Hotta K, Kato K, Nakagawa J, et al. Quality of life of survivors of malignant pleural mesothelioma in Japan: a cross sectional study. BMC Cancer. 2018;18(1):350.
Guglielmucci F, Franzoi IG, Bonafede M, Borgogno FV, Grosso F, Granieri A. “The Less I Think About It, the Better I Feel”: A Thematic Analysis of the Subjective Experience of Malignant Mesothelioma Patients and Their Caregivers. Front Psychol. 2018;9:205.
Bonafede M, Ghelli M, Corfiati M, Rosa V, Guglielmucci F, Granieri A, et al. The psychological distress and care needs of mesothelioma patients and asbestos-exposed subjects: A systematic review of published studies. Am J Ind Med. 2018;61(5):400-12.
Sherborne V, Seymour J, Taylor B, Tod A. What are the psychological effects of mesothelioma on patients and their carers? A scoping review. Psychooncology. 2020.
EORTC. Questionnaires: Quality of life of cancer patients. EORTC Quality of Life: European Organization for Research and Treatment of Cancer (EORTC). p. https://qol.eortc.org/questionnaire/eortc-qlq-c30/.
Miyashita M, Wada M, Morita T, Ishida M, Onishi H, Tsuneto S, et al. Development and validation of the Comprehensive Quality of Life Outcome (CoQoLo) inventory for patients with advanced cancer. BMJ Support Palliat Care. 2019;9(1):75-83.
Odgerel CO, Takahashi K, Sorahan T, Driscoll T, Fitzmaurice C, Yoko OM, et al. Estimation of the global burden of mesothelioma deaths from incomplete national mortality data. Occup Environ Med. 2017;74(12):851-8.
Nagamatsu Y, Natori Y, Yanai H, Horiuchi S. Impact of a nursing education program about caring for patients in Japan with malignant pleural mesothelioma on nurses’ knowledge, difficulties and attitude: a randomized control trial. Nurse Educ Today. 2014;34(7):1087-93.
AIHW. Mesothelioma in Australia 2019. In: infocus, editor. Australian Mesothelioma Registry: Australian Institute of Health and Welfare; 2020.
Cavanagh A. The total number of diagnoses and hospitalisations for diseases of the respiratory system (ICD-12) in New Zealand in the 2-017-2018 year. The request may be refined to the total number of hospitalisations only, to exclude diagnoses.” In: Ministry of Health NZ, editor.: Ministry of Health, New Zeland; 2018. p. 13.
Fennell D, A. . Unmet needs and future outlook of mesothelioma management. 2019 20 June 2019. In: (Mesothelioma [Internet]. Springer Cham. Available from: https://doi.org/10.1007/978-3-030-16884-1_23.
Hughes N, Arber A. The lived experience of patients with pleural mesothelioma. Int J Palliat Nurs. 2008;14(2):66-71.
Moore S, Teehan C, Cornwall A, Ball K, Thomas J. ‘Hands of Time’: the experience of establishing a support group for people affected by mesothelioma. Eur J Cancer Care (Engl). 2008;17(6):585-92.
Harrison M, Gardiner C, Taylor B, Ejegi-Memeh S, Darlison L. Understanding the palliative care needs and experiences of people with mesothelioma and their family carers: An integrative systematic review. Palliat Med. 2021;35(6):1039-51.
Henshall C, Davey Z, Walthall H, Ball H, Shahidi M, Park J, et al. Recommendations for improving follow-up care for patients with mesothelioma: a qualitative study comprising documentary analysis, interviews and consultation meetings. BMJ Open. 2021;11(1):e040679.